

Ischemic Stroke Severity and Mortality in Patients With and Without Atrial Fibrillation
- PMID: 35156393
- PMCID: PMC9245802
- DOI: 10.1161/JAHA.121.022638
Ischemic Stroke Severity and Mortality in Patients With and Without Atrial Fibrillation
Erratum in
-
Correction to: Ischemic Stroke Severity and Mortality in Patients With and Without Atrial Fibrillation.J Am Heart Assoc. 2022 Aug 16;11(16):e020613. doi: 10.1161/JAHA.121.020613. Epub 2022 Jul 5. J Am Heart Assoc. 2022. PMID: 35862199 Free PMC article. No abstract available.
Abstract
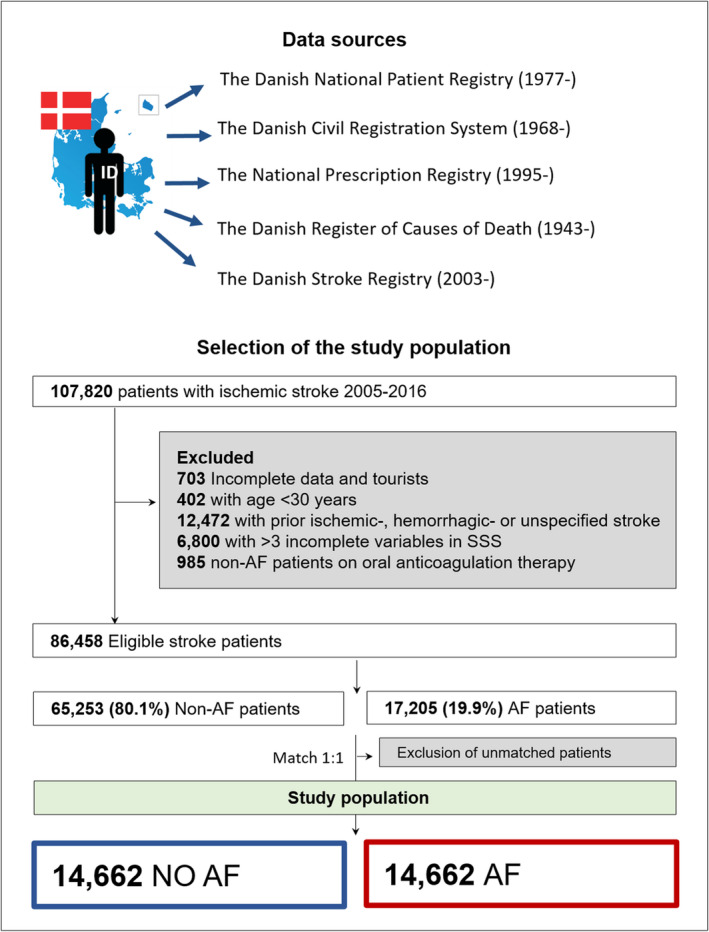
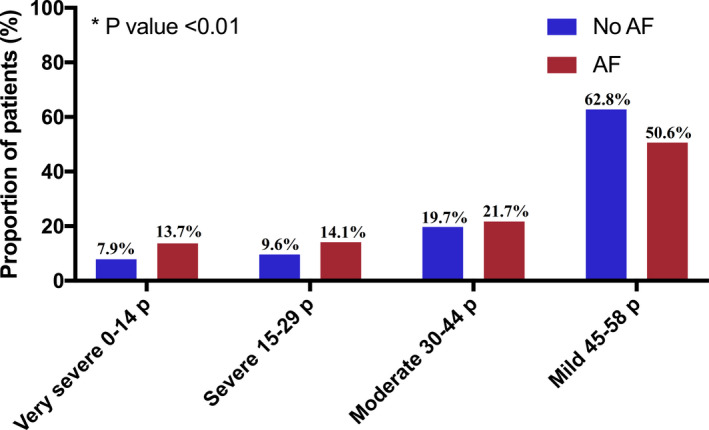
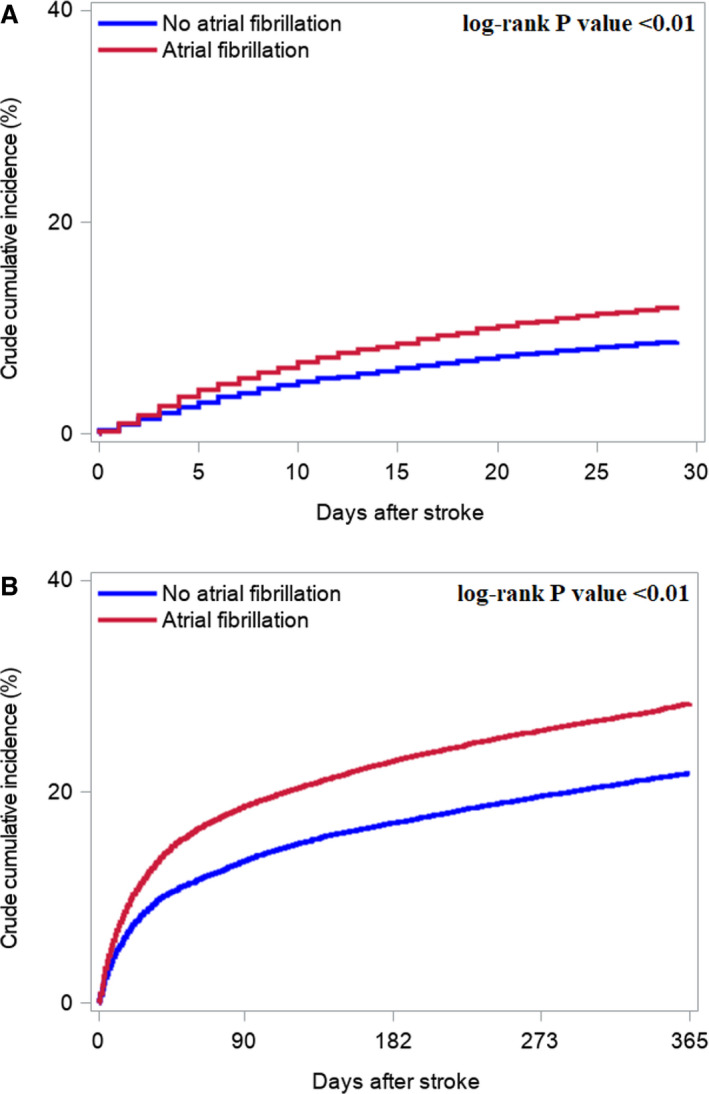
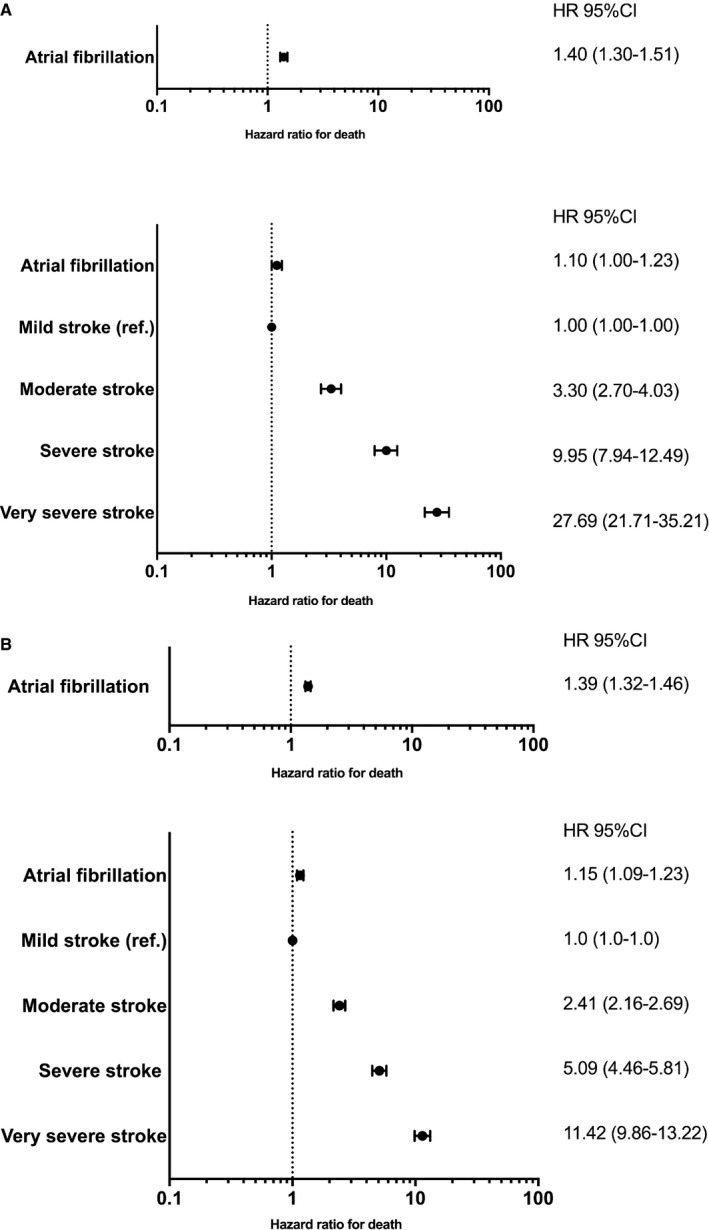
Background Our objective was to investigate stroke severity and subsequent rate of mortality among patients with and without atrial fibrillation (AF). Contemporary data on stroke severity and prognosis in patients with AF are lacking. Methods and Results First-time ischemic stroke patients from the Danish Stroke Registry (January 2005-December 2016) were included in an observational study. Patients with AF were matched 1:1 by sex, age, calendar year, and CHA2DS2-VASc score with patients without AF. Stroke severity was determined by the Scandinavian Stroke Scale (0-58 points). The rate of death was estimated by Kaplan-Meier plots and multivariable Cox regression. Among 86 458 identified patients with stroke, 17 205 had AF. After matching, 14 662 patients with AF and 14 662 patients without AF were included (51.8% women; median age, 79.6 years [25th-75th percentile, 71.8-86.0]). More patients with AF had very severe stroke (0-14 points) than patients without AF (13.7% versus 7.9%, P<0.01). The absolute rates of 30-day and 1-year mortality were significantly higher for patients with AF (12.1% and 28.4%, respectively) versus patients without AF (8.7% and 21.8%, respectively). This held true in adjusted models for 30-day mortality (hazard ratio [HR], 1.40 [95% CI, 1.30-1.51]). However, this association became nonsignificant when additionally adjusting for stroke severity (HR, 1.10 [95% CI, 1.00-1.23]). AF was associated with a higher rate of 1-year mortality (HR, 1.39 [95% CI, 1.32-1.46]), although it was mediated by stroke severity (HR, 1.15 [95% CI, 1.09-1.23], model including stroke severity). Conclusions In a contemporary nationwide cohort of patients with ischemic stroke, patients with AF had more severe strokes and higher mortality than patients without AF. The difference in mortality was mainly driven by stroke severity.
Keywords: atrial fibrillation; epidemiology; ischemic stroke; severity; stroke severity.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
