

Ventilatory efficiency slope is associated with cardiopulmonary complications after thoracoscopic anatomical lung resection
- PMID: 35157073
- PMCID: PMC9252121
- DOI: 10.1093/icvts/ivac039
Ventilatory efficiency slope is associated with cardiopulmonary complications after thoracoscopic anatomical lung resection
Abstract
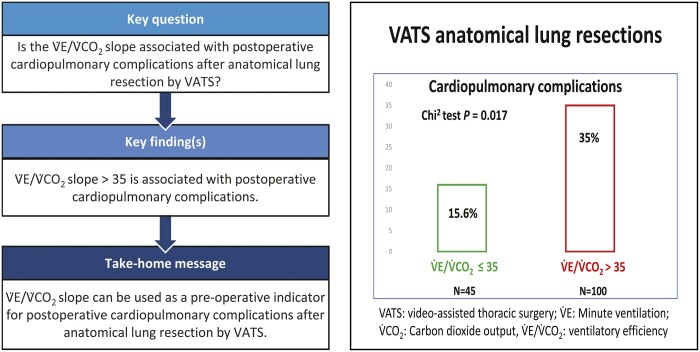
Objectives: The aim of this study was to identify whether steeper V.E/V. CO2 slope was associated with cardiopulmonary complications (CPC) after anatomical resection by video-assisted thoracic surgery. Long-term survival was analysed as secondary outcome.
Methods: We reviewed the files of all consecutive patients who underwent pulmonary anatomical resections by video-assisted thoracic surgery between January 2010 and October 2020 at the Centre for Thoracic Surgery of Western Switzerland. Logistic regression was used to investigate the risk of CPC associated with the V.E/V.CO2 slope and other possible confounders. Survival was analysed with Kaplan-Meier curves. Risk factors associated with survival were analysed with a Cox proportional hazards model.
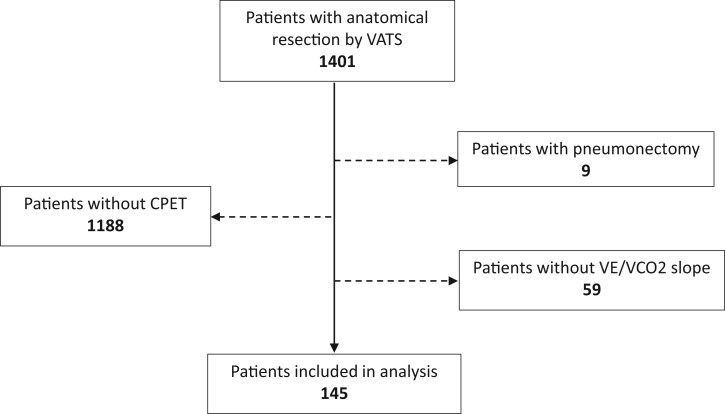
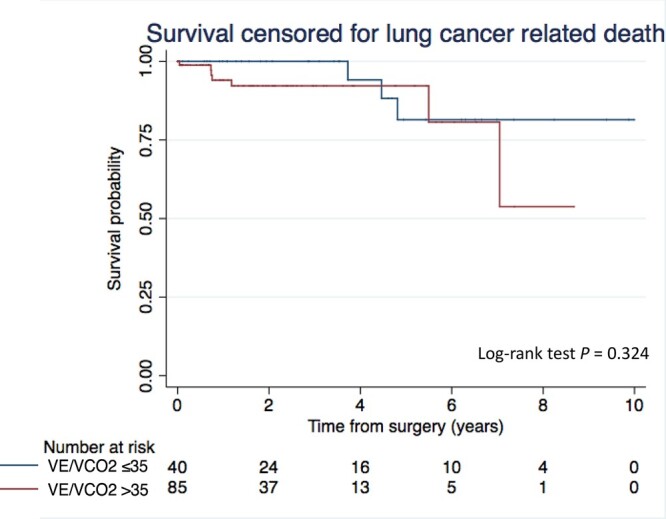
Results: The V.E/V.CO2 slope data were available for 145 patients [F/M: 66/79; mean age (standard deviation): 65.8 (8.9)], which were included in the analysis. Patients underwent anatomical resection [lobectomy (71%) or segmentectomy (29%)] mainly for lung cancer (96%). CPC and all-cause 90-day mortality were 29% and 1%, respectively. The mean (standard deviation) percentage of the predicted V.O2peak was 70% (17). Maximum effort during cardiopulmonary exercise test was reached in only 31% of patients. The V.E/V.CO2 slope (standard deviation) was not different if the maximum effort was reached or not [39 (6) vs 37 (7), P = 0.21]. V.E/V.CO2 slope >35 was associated with an increased risk of CPC (odds ratio 2.9, 95% confidence interval 1.2, 7.2, P = 0.020). V.E/V.CO2 slope >35 was not associated with shorter survival censored for lung cancer-related death.
Conclusions: V . E/V.CO2 slope >35 is significantly associated with postoperative CPC after anatomical resections by video-assisted thoracic surgery.
Clinical registration number cer-vd (switzerland): Project ID: 2021-00620.
Keywords: Anatomical lung resection; Lung cancer; Minute ventilation-to-carbon dioxide output slope; Postoperative complications; Ventilatory efficiency; Video-assisted thoracic surgery.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Bendixen M, Jørgensen OD, Kronborg C, Andersen C, Licht PB.. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomized controlled trial. Lancet Oncol 2016;17:836–44. - PubMed
-
- Falcoz PE, Puyraveau M, Thomas PA, Decaluwe H, Hürtgen M, Petersen RH. et al. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: a propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur J Cardiothorac Surg 2016;49:602–9. - PubMed
-
- Brunelli A, Kim AW, Berger KI, Addrizzo-Harris DJ.. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e166S–90S. - PubMed
-
- Brunelli A, Charloux A, Bolliger CT, Rocco G, Sculier J-P, Varela G. et al.; European Respiratory Society and European Society of Thoracic Surgeons joint task force on fitness for radical therapy. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J 2009;34:17–41. - PubMed
-
- Bolliger CT, Jordan P, Solèr M, Stulz P, Grädel E, Skarvan K. et al. Exercise capacity as a predictor of postoperative complications in lung resection candidates. Am J Respir Crit Care Med 1995;151:1472–80. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
