

A case of pathologically confirmed streptococcal infection-related IgA vasculitis with associated glomerulonephritis and leukocytoclastic cutaneous vasculitis
- PMID: 35157249
- PMCID: PMC9343489
- DOI: 10.1007/s13730-022-00684-4
A case of pathologically confirmed streptococcal infection-related IgA vasculitis with associated glomerulonephritis and leukocytoclastic cutaneous vasculitis
Abstract
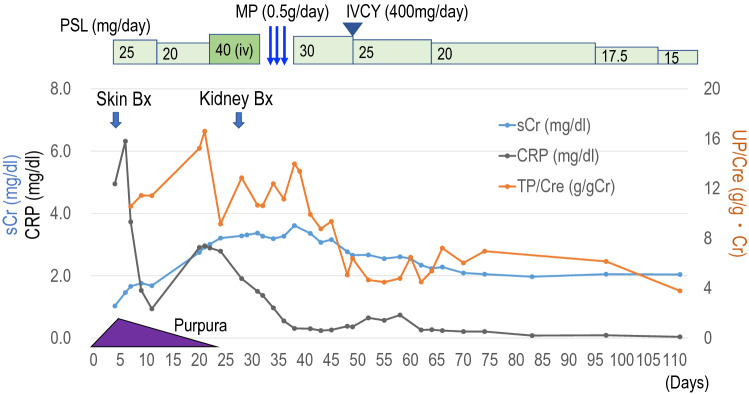
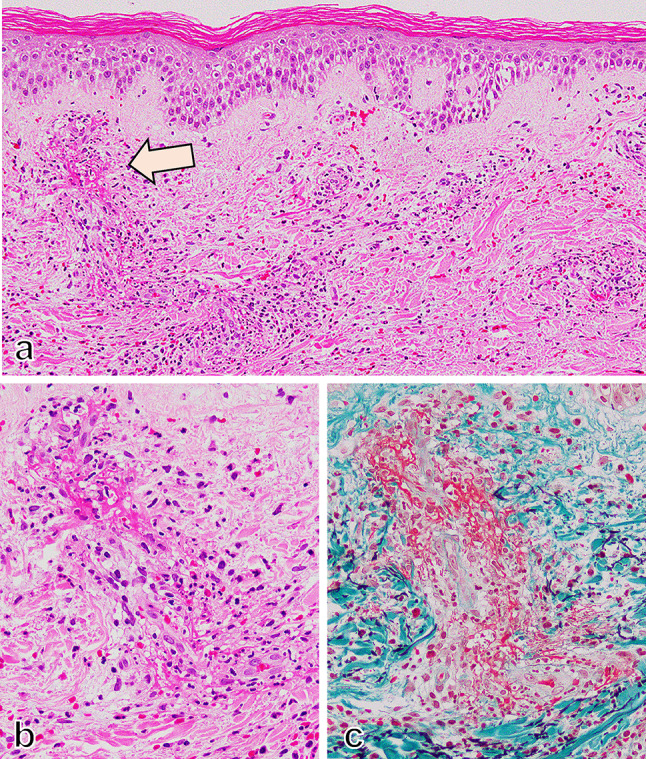
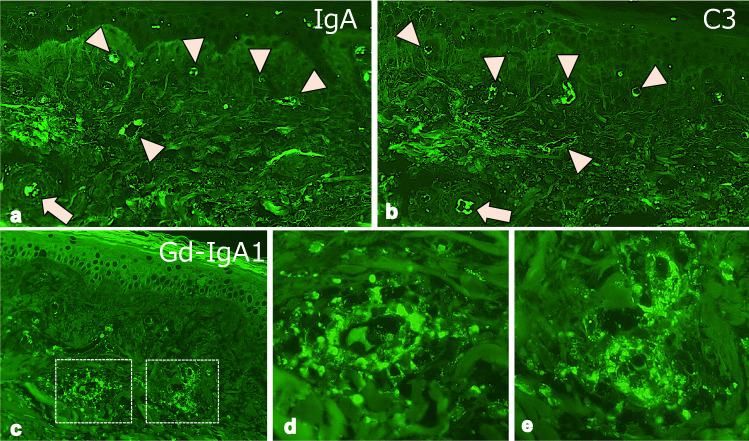
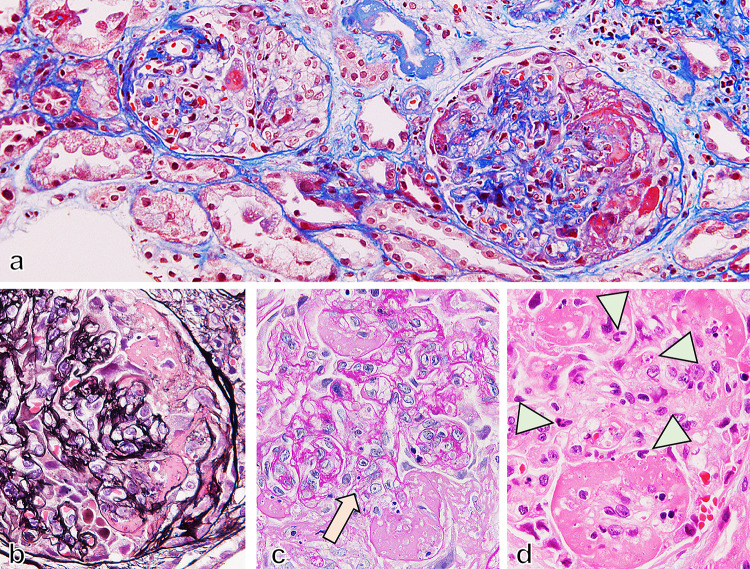
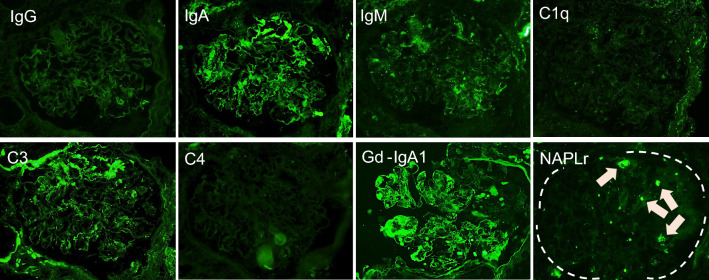
We report the case of an 80 year-old woman who developed bilateral lower extremity purpura and renal impairment with proteinuria a few days after a transient fever (day 0). High levels of both anti-streptolysin-O antibody (ASO) and anti-streptokinase antibody (ASK), as well as low levels of coagulation factor XIII in serum were noted. Skin biopsy was performed and showed a leukocytoclastic vasculitis with deposition of IgA and C3 in the cutaneous small vessels, indicating IgA vasculitis in the skin. After initiation of oral prednisolone, the skin lesions showed significant improvement. However, renal function and proteinuria gradually worsened from day 12. Kidney biopsy was performed on day 29, which demonstrated a necrotizing and crescentic glomerulonephritis with mesangial deposition of IgA and C3. In addition, the deposition of galactose-deficient IgA1 (Gd-IgA1) was positive on glomeruli and cutaneous small vessels, indicating that the purpura and glomerulonephritis both shared the same Gd-IgA1-related pathogenesis. In addition, the association between the acute streptococcal infection and the IgA vasculitis was confirmed by the deposition of nephritis-associated plasmin receptor (NAPlr) in glomeruli. The patient was treated with steroid pulse and intravenous cyclophosphamide, in addition to the oral prednisolone treatment. Renal function and proteinuria gradually improved, but did not completely recover, as is typically seen with courses of IgA vasculitis in the elderly. In this case, the streptococcal infectionrelated IgA vasculitis was confirmed pathologically by the deposition of both NAPlr and Gd-IgA1 in glomeruli, as well as Gd-IgA1 in the cutaneous small vessels.
Keywords: Gd-IgA1; IgA vasculitis; NAPlr; Streptococcal infection.
© 2022. The Author(s) under exclusive licence to The Japan Society of Nephrology.
Conflict of interest statement
The authors have declared that no conflict of interest exists.
Figures
References
-
- Yumura W, Kobayashi S, Suka M, Hayashi T, Ito S, Nagafuchi H, et al. Assessment of the Birmingham vasculitis activity score in patients with MPO-ANCA-associated vasculitis: sub-analysis from a study by the Japanese Study Group for MPO-ANCA-associated vasculitis. Mod Rheumatol. 2014;24(2):304–309. doi: 10.3109/14397595.2013.854075. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
