

Hepatic lymphatic vascular system in health and disease
- PMID: 35157960
- PMCID: PMC9870070
- DOI: 10.1016/j.jhep.2022.01.025
Hepatic lymphatic vascular system in health and disease
Abstract
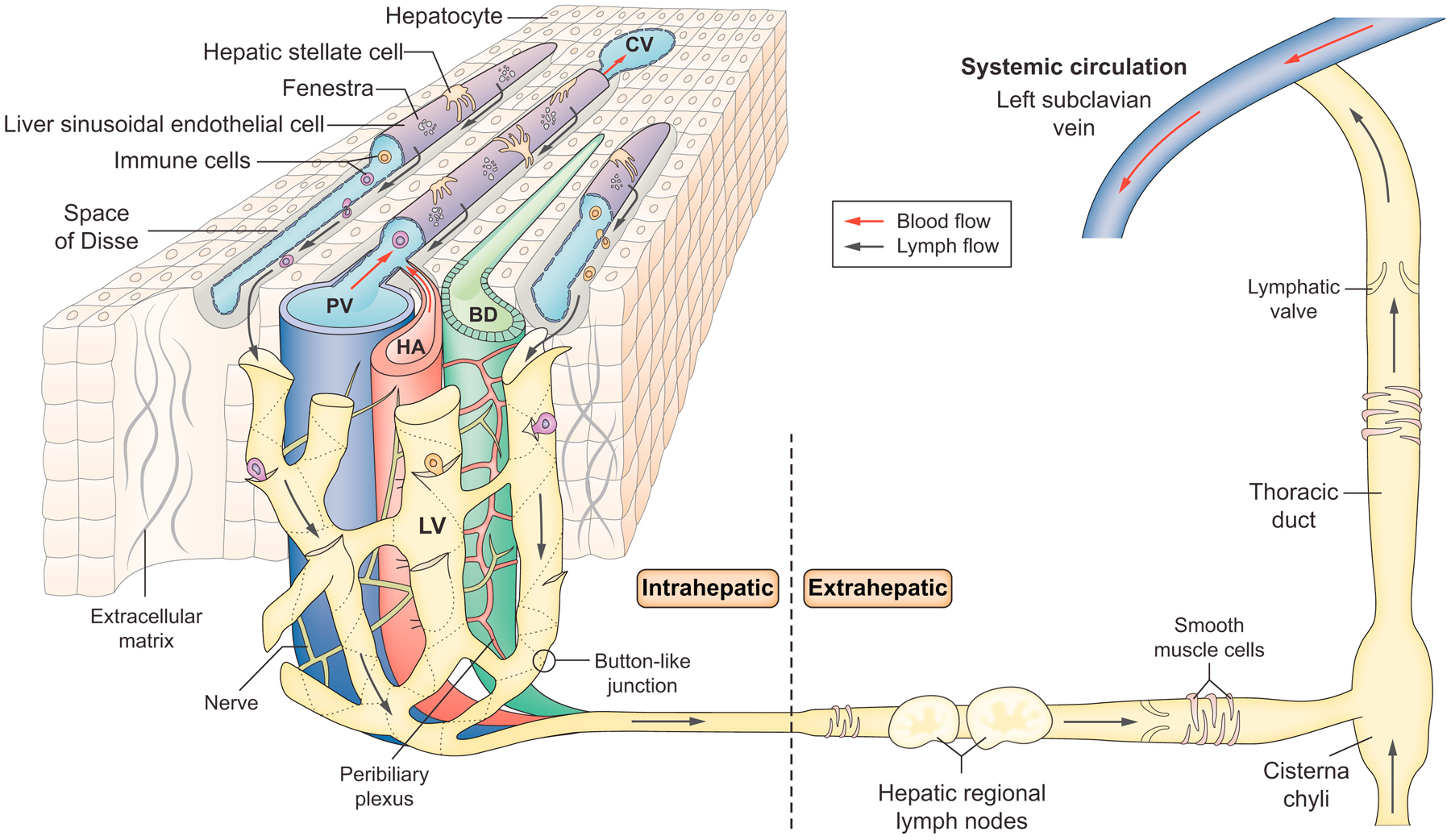
In recent years, significant advances have been made in the study of lymphatic vessels with the identification of their specific markers and the development of research tools that have accelerated our understanding of their role in tissue homeostasis and disease pathogenesis in many organs. Compared to other organs, the lymphatic system in the liver is understudied despite its obvious importance for hepatic physiology and pathophysiology. In this review, we describe fundamental aspects of the hepatic lymphatic system and its role in a range of liver-related pathological conditions such as portal hypertension, ascites formation, malignant tumours, liver transplantation, congenital liver diseases, non-alcoholic fatty liver disease, and hepatic encephalopathy. The article concludes with a discussion regarding the modulation of lymphangiogenesis as a potential therapeutic strategy for liver diseases.
Keywords: Lymphangiogenesis; VEGFs; liver fibrosis; liver transplantation; portal hypertension.
Copyright © 2022 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures



References
-
- Morris B The hepatic and intestinal contributions to the thoracic duct lymph. Q J Exp Physiol Cogn Med Sci 1956;41:318–325. - PubMed
-
- Cain JC, Grindlay JH, et al. Lymph from liver and thoracic duct; an experimental study. Surg Gynecol Obstet 1947;85:558–562. - PubMed
-
- Mobley WP, Kintner K, Witte CL, Witte MH. Contribution of the liver to thoracic duct lymph flow in a motionless subject. Lymphology 1989;22:81–84. - PubMed
-
- Ohtani O, Ohtani Y. Lymph circulation in the liver. Anat Rec (Hoboken) 2008;291:643–652. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
