

Incidence and Risk Factors of Cancer in the Anal Transitional Zone and Ileal Pouch following Surgery for Ulcerative Colitis and Familial Adenomatous Polyposis
- PMID: 35158797
- PMCID: PMC8833833
- DOI: 10.3390/cancers14030530
Incidence and Risk Factors of Cancer in the Anal Transitional Zone and Ileal Pouch following Surgery for Ulcerative Colitis and Familial Adenomatous Polyposis
Abstract
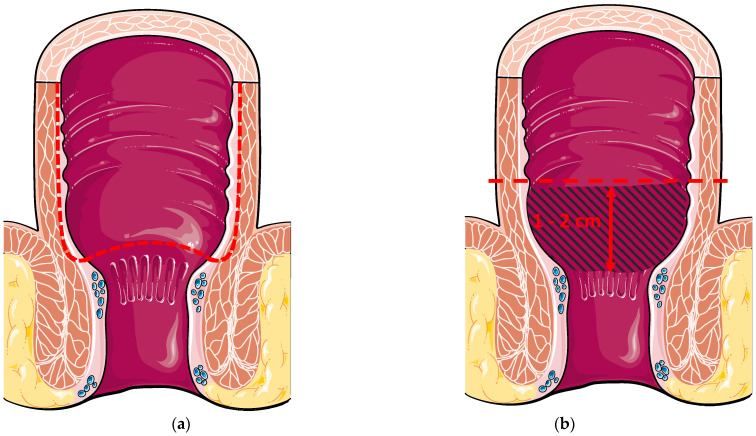
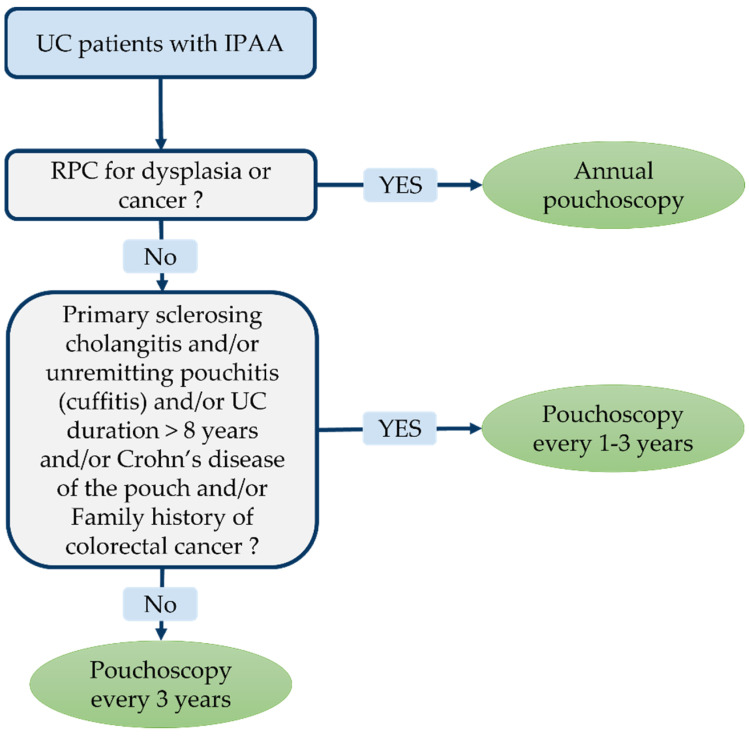
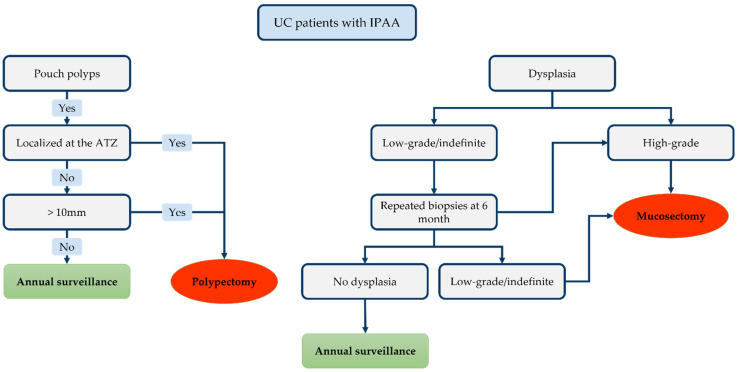
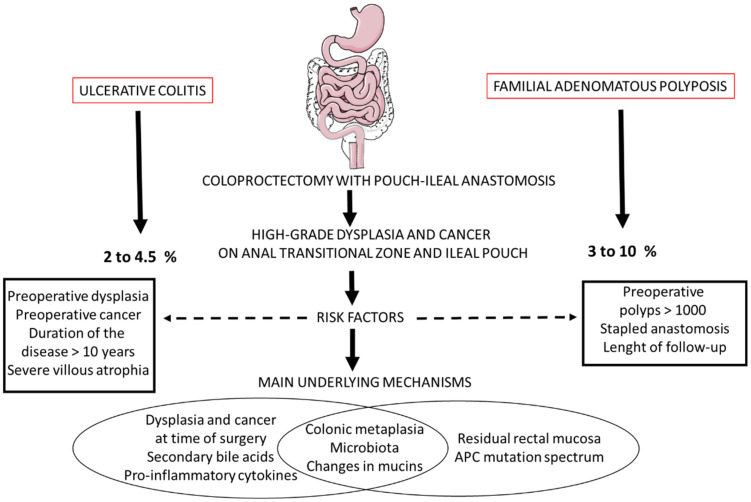
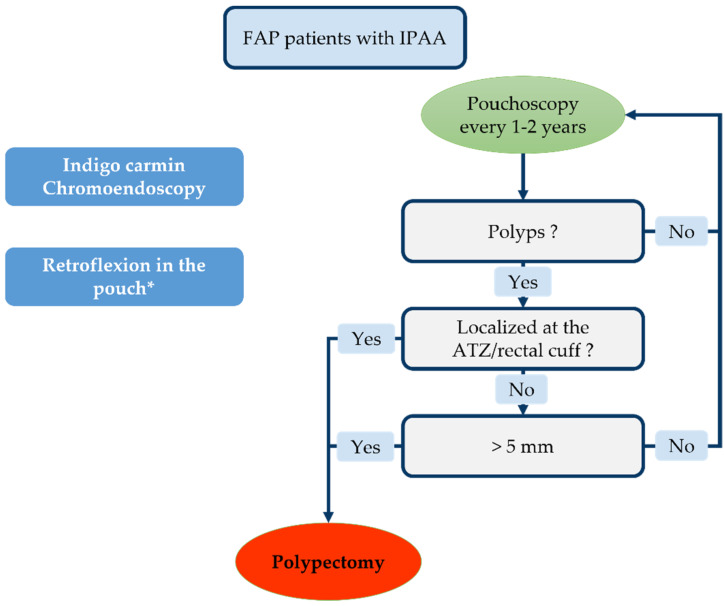
Proctocolectomy with ileal pouch-anal anastomosis is the intervention of choice for ulcerative colitis and familial adenomatous polyposis requiring surgery. One of the long-term complications is pouch cancer, having a poor prognosis. The risk of high-grade dysplasia and cancer in the anal transitional zone and ileal pouch after 20 years is estimated to be 2 to 4.5% and 3 to 10% in ulcerative colitis and familial polyposis, respectively. The risk factors for ulcerative colitis are the presence of pre-operative dysplasia or cancer, disease duration > 10 years and severe villous atrophy. For familial polyposis, the risk factors are the number of pre-operative polyps > 1000, surgery with stapled anastomosis and the duration of follow-up. In the case of ulcerative colitis, a pouchoscopy should be performed annually if one of the following is present: dysplasia and cancer at surgery, primary sclerosing cholangitis, villous atrophy and active pouchitis (every 5 years without any of these factors). In the case of familial polyposis, endoscopy is recommended every year including chromoendoscopy. Even if anal transitional zone and ileal pouch cancers seldom occur following proctectomy for ulcerative colitis and familial adenomatous polyposis, the high mortality rate associated with this complication warrants endoscopic monitoring.
Keywords: anal transitional zone cancer; familial adenomatous polyposis; high grade dysplasia; ileal pouch; ulcerative colitis.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Frolkis A.D., Dykeman J., Negrón M.E., Debruyn J., Jette N., Fiest K.M., Frolkis T., Barkema H.W., Rioux K.P., Panaccione R., et al. Risk of Surgery for Inflammatory Bowel Diseases Has Decreased over Time: A Systematic Review and Meta-Analysis of Population-Based Studies. Gastroenterology. 2013;145:996–1006. doi: 10.1053/j.gastro.2013.07.041. - DOI - PubMed
-
- Magro F., Gionchetti P., Eliakim R., Ardizzone S., Armuzzi A., Barreiro-de Acosta M., Burisch J., Gecse K.B., Hart A.L., Hindryckx P., et al. Third European Evidence-Based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-Intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-Anal Pouch Disorders. J. Crohns Colitis. 2017;11:649–670. doi: 10.1093/ecco-jcc/jjx008. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
