

External Validation of the RETREAT Score for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation
- PMID: 35158898
- PMCID: PMC8833722
- DOI: 10.3390/cancers14030630
External Validation of the RETREAT Score for Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation
Abstract
Background: We aimed to externally validate the performance of the RETREAT score in a European population.
Methods: This single center retrospective cohort study enrolled all consecutive patients with HCC who underwent LT between 1989 and 2019. The performance of RETREAT was assessed in the overall population and after stratification between being within or beyond the Milan criteria based on the explant pathology report. Recurrence probabilities were estimated by using the Kaplan-Meier method and compared by log-rank test.
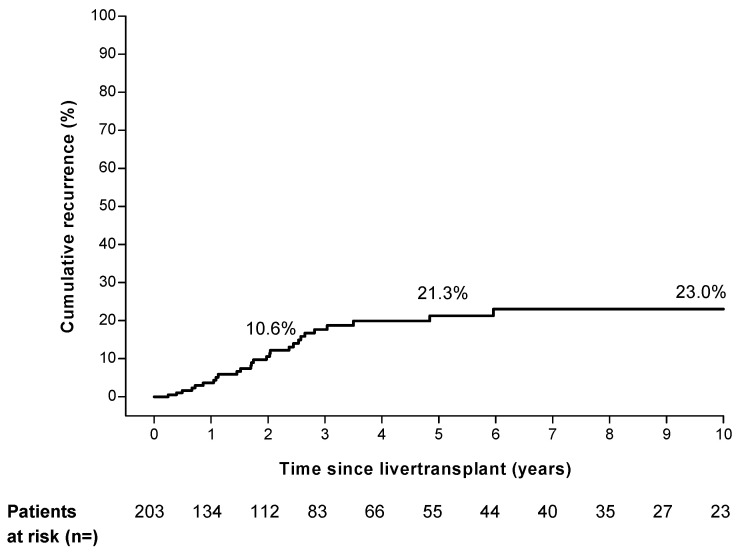
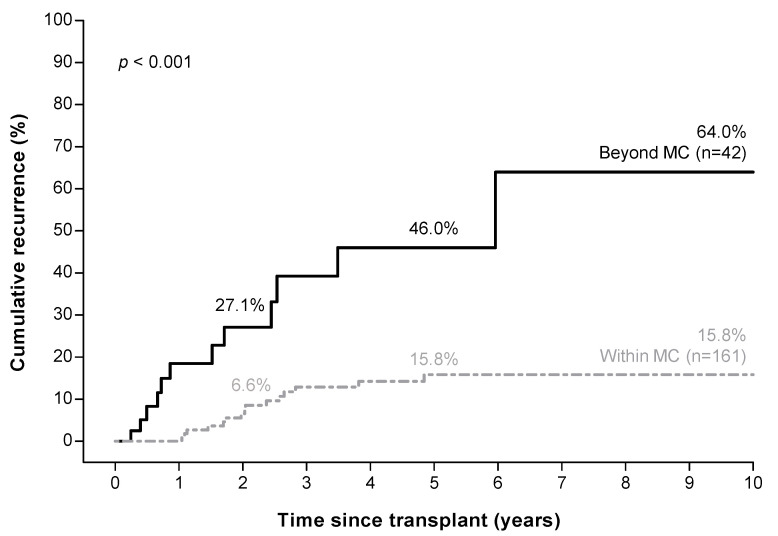
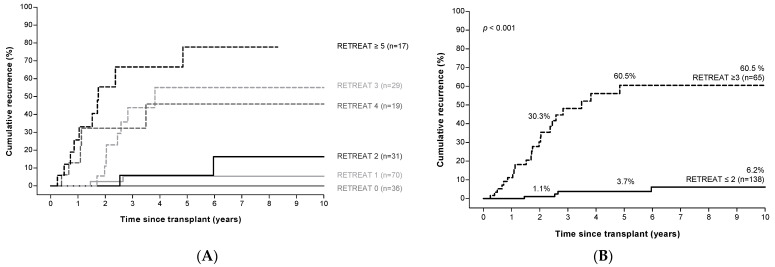
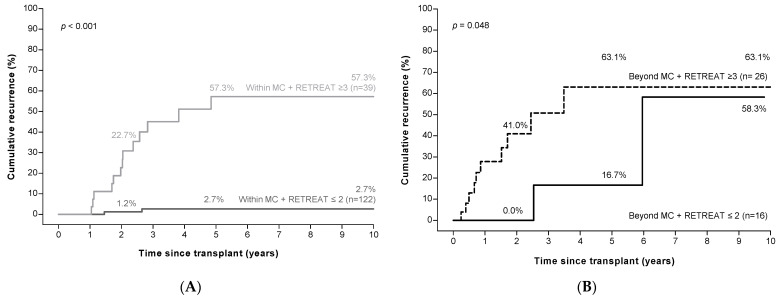
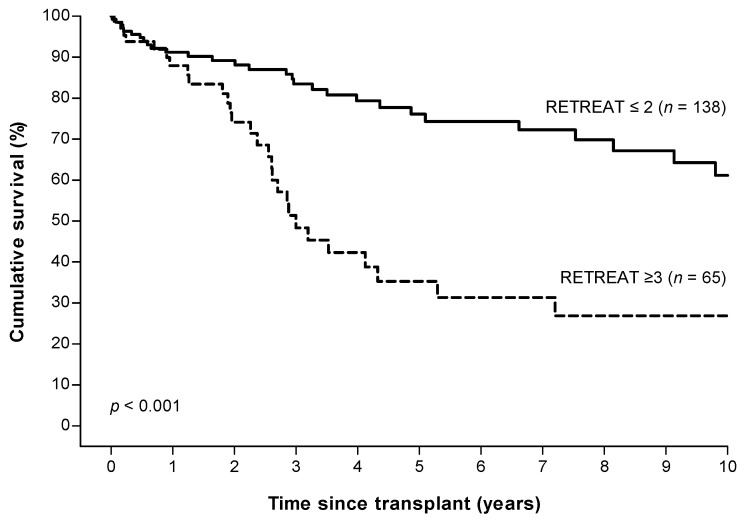
Results: We studied 203 patients; 42 patients were beyond the Milan criteria based on explant pathology. The median follow-up was 26.8 months (IQR 7.2-60.7). Overall cumulative HCC recurrence rates were 10.6%, 21.3%, and 23.0% at 2, 5, and 10 years, with the majority of recurrences extrahepatic and at multiple sites. Higher RETREAT scores were associated with higher recurrence rates, with a 10-year recurrence rate of 60.5% in patients with RETREAT ≥ 3 (n = 65), compared to 6.2% in those with RETREAT ≤2 (n = 138; p < 0.001). HCC recurrence rates were even lower in patients within the Milan criteria who also had a low RETREAT score (n = 122; 2.7% at 10 years).
Conclusion: Low RETREAT scores identify patients at low risk of HCC recurrence after LT in patients within the Milan criteria based on explant pathology.
Keywords: Milan criteria; hepatocellular carcinoma; liver neoplasms; liver transplantation; recurrence; risk score.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Clavien P.A., Lesurtel M., Bossuyt P.M., Gores G.J., Langer B., Perrier A., Group O.L.T.f.H.C. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012;13:e11–e22. doi: 10.1016/S1470-2045(11)70175-9. - DOI - PMC - PubMed
-
- Mazzaferro V., Regalia E., Doci R., Andreola S., Pulvirenti A., Bozzetti F., Montalto F., Ammatuna M., Morabito A., Gennari L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996;334:693–699. doi: 10.1056/NEJM199603143341104. - DOI - PubMed
-
- Bodzin A.S., Lunsford K.E., Markovic D., Harlander-Locke M.P., Busuttil R.W., Agopian V.G. Predicting mortality in patients developing recurrent hepatocellular carcinoma after liver transplantation: Impact of treatment modality and recurrence characteristics. Ann. Surg. 2017;266:118–125. doi: 10.1097/SLA.0000000000001894. - DOI - PubMed
LinkOut - more resources
Full Text Sources
