

MRI-Guided Online Adaptive Stereotactic Body Radiation Therapy of Liver and Pancreas Tumors on an MR-Linac System
- PMID: 35158984
- PMCID: PMC8833602
- DOI: 10.3390/cancers14030716
MRI-Guided Online Adaptive Stereotactic Body Radiation Therapy of Liver and Pancreas Tumors on an MR-Linac System
Abstract
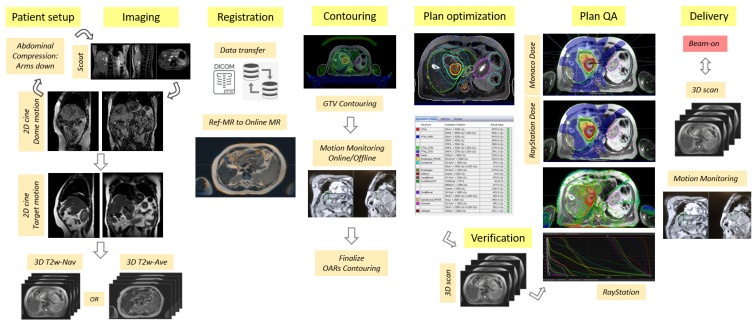
Purpose: To describe a comprehensive workflow for MRI-guided online adaptive stereotactic body radiation therapy (SBRT) specific to upper gastrointestinal cancer patients with abdominal compression on a 1.5T MR-Linac system. Additionally, we discuss the workflow's clinical feasibility and early experience in the case of 16 liver and pancreas patients.
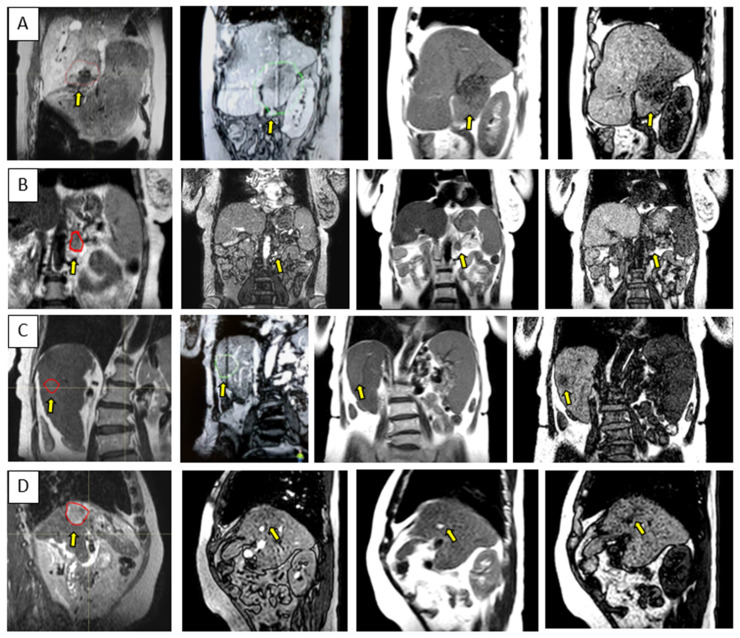
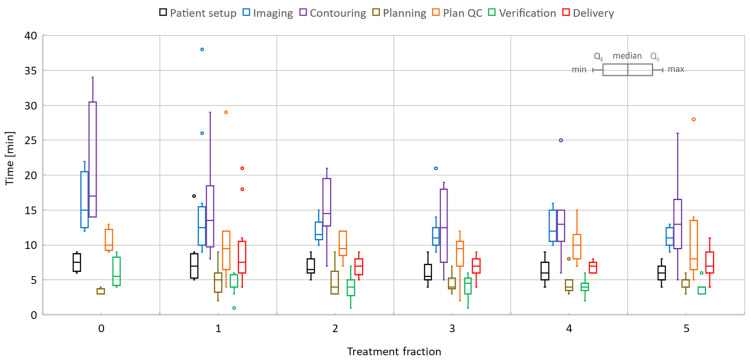
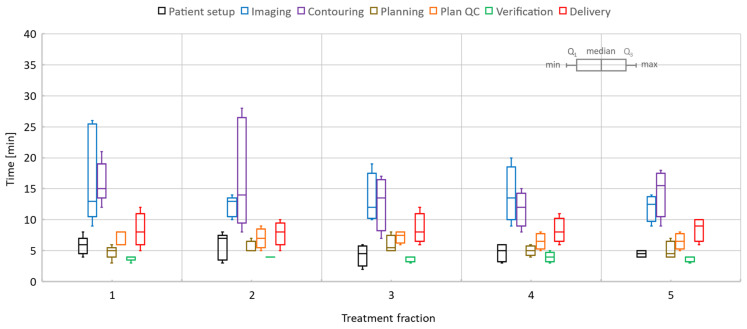
Methods: Eleven patients with liver cancer and five patients with pancreas cancer were treated with online adaptive MRI-guidance under abdominal compression. Two liver patients received single-fraction treatments; the remainder plus all pancreas cancer patients received five fractions. A total of 65 treatment sessions were investigated to provide analytics relevant to the online adaptive processes. The quantification of target and organ motion as well as definition and validation of internal target volume (ITV) margins were performed via multi-contrast imaging provided by three different 2D cine sequences. The plan generation was driven by full re-optimization strategies and using T2-weighted 3D image series acquired by means of a respiratory-triggered exhale phase or a time-averaged imaging protocol. As a pre-requisite for the clinical development of the procedure, the image quality was thoroughly investigated via phantom measurements and numerical simulations specific to upper abdominal sites. The delivery of the online adaptive treatments was facilitated by real-time monitoring with 2D cine imaging.
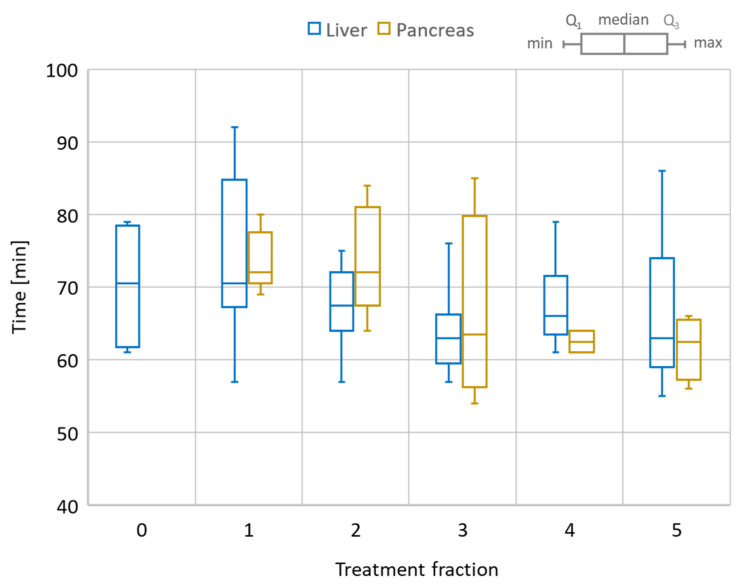
Results: Liver 1-fraction and 5-fraction online adaptive session time were on average 80 and 67.5 min, respectively. The total session length varied between 70-90 min for a single fraction and 55-90 min for five fractions. The pancreas sessions were 54-85 min long with an average session time of 68.2 min. Target visualization on the 2D cine image data varied per patient, with at least one of the 2D cine sequences providing sufficient contrast to confidently identify its location and confirm reproducibility of ITV margins. The mean/range of absolute and relative dose values for all treatment sessions evaluated with ArcCheck were 90.6/80.9-96.1% and 99/95.4-100%, respectively.
Conclusion: MR-guidance is feasible for liver and pancreas tumors when abdominal compression is used to reduce organ motion, improve imaging quality, and achieve a robust intra- and inter-fraction patient setup. However, the treatment length is significantly longer than for the conventional linac, and patient compliance is paramount for the successful completion of the treatment. Opportunities for reducing the online adaptive session time should be explored. As the next steps, dose-of-the-day and dose accumulation analysis and tools are needed to enhance the workflow and to help further refine the online re-planning processes.
Keywords: HCC; MR image distortions; MR-Linac; MR-guided radiation therapy; MRI; MRIgRT; MRgRT; SBRT; liver metastases; numerical simulations; pancreas; susceptibility.
Conflict of interest statement
A.H.—Non-financial leadership of the liver tumor site group at Elekta MRL Consortium. The rest of the authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
