

Oral Immune-Related Adverse Events Caused by Immune Checkpoint Inhibitors: Salivary Gland Dysfunction and Mucosal Diseases
- PMID: 35159059
- PMCID: PMC8834130
- DOI: 10.3390/cancers14030792
Oral Immune-Related Adverse Events Caused by Immune Checkpoint Inhibitors: Salivary Gland Dysfunction and Mucosal Diseases
Abstract
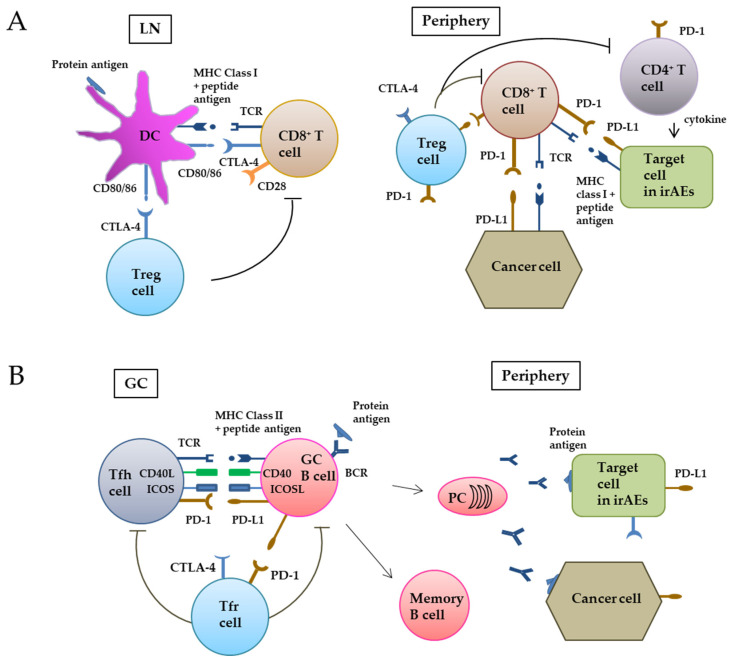
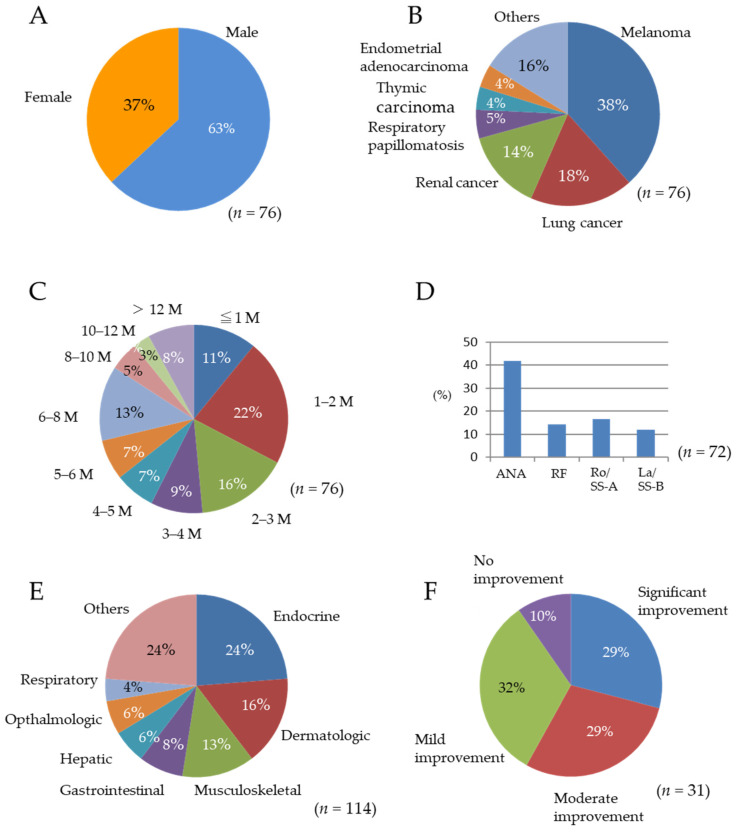
Conventional chemotherapy and targeted therapies have limited efficacy against advanced head and neck squamous cell carcinoma (HNSCC). The immune checkpoint inhibitors (ICIs) such as antibodies against CTLA-4, PD-1, and PD-L1 interrupt the co-inhibitory pathway of T cells and enhance the ability of CD8+ T cells to destroy tumors. Even in advanced HNSCC patients with recurrent diseases and distant metastasis, ICI therapy shows efficiency and become an effective alternative to conventional chemotherapy. However, as this therapy releases the immune tolerance state, cytotoxic CD8+ T cells can also attack organs and tissues expressing self-antigens that cross-react with tumor antigens and induce immune-related adverse events (irAEs). When patients with HNSCC are treated with ICIs, autoimmune diseases occur in multiple organs including the skin, digestive tract, endocrine system, liver, and respiratory tract. Treatment of various malignancies, including HNSCC, with ICIs may result in the appearance of oral irAEs. In the oral cavity, an oral lichenoid reaction (OLR) and pemphigoid develop. Sicca syndrome also occurs in association with ICIs, affecting the salivary glands to induce xerostomia. It is necessary to elucidate the pathogenic mechanisms of these intractable diseases that are not seen with conventional therapy. Early diagnosis and appropriate approaches to irAEs are needed for efficient treatment of advanced HNSCC by ICIs.
Keywords: Sicca syndrome; cellular and humoral tumor immunity; head and neck squamous cell carcinoma; immune checkpoint inhibitor; immune-related adverse event; oral cavity; oral lichenoid reaction; pemphigoid.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Jakobi A., Lühr A., Stützer K., Bandurska-Luque A., Löck S., Krause M., Baumann M., Perrin R., Richter C. Increase in Tumor Control and Normal Tissue Complication Probabilities in Advanced Head-and-Neck Cancer for Dose-Escalated Intensity-Modulated Photon and Proton Therapy. Front. Oncol. 2015;5:256. doi: 10.3389/fonc.2015.00256. - DOI - PMC - PubMed
-
- Yura Y., Tada S., Fujita Y., Hamada M. Current treatment, particle radiotherapy, and boron neutron capture therapy for advanced oral cancer in patients. Oral Sci. Int. 2019;16:49–68. doi: 10.1002/osi2.1014. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
