

Oncogenic Alterations in Histologically Negative Lymph Nodes Are Associated with Prognosis of Patients with Stage I Lung Adenocarcinoma
- PMID: 35159091
- PMCID: PMC8834139
- DOI: 10.3390/cancers14030824
Oncogenic Alterations in Histologically Negative Lymph Nodes Are Associated with Prognosis of Patients with Stage I Lung Adenocarcinoma
Abstract
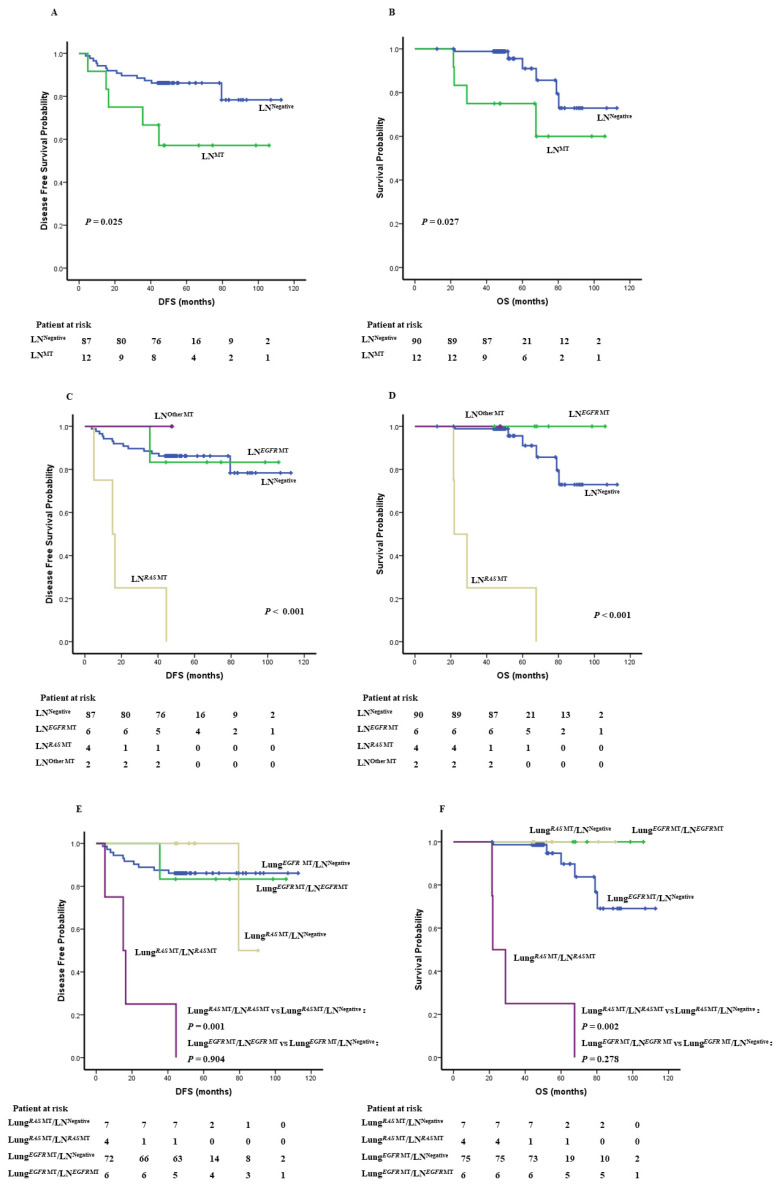
Background: Survival of patients with stage I non-small cell lung cancer (NSCLC) varies greatly. We sought to explore whether presence of oncogenic alterations in histologically-negative lymph nodes (LNs) can be of prognostic significance in stage I lung adenocarcinoma (LUAD). Methods: Genomic analysis of oncogenic alterations was applied to 123 stage I LUAD tumors. The same genomic variants identified in primary tumors were examined in corresponding histologically-negative LNs. Results: A total of 102 (82.9%) patients had at least one canonical oncogenic alteration detected in primary tumors, and 57 LNs from 12 patients (11.8%) were found to carry the identical oncogenic alterations detected in the corresponding primary tumor tissues, including EGFR mutations (six cases), KRAS mutations (three cases), ALK fusion (one case), BRAF mutation (one case) and HER2 & NRAS co-mutations (one case). None of these LNs was found to have occult tumor cells by routine pathological assessment or immunohistochemistry staining using antibodies against pan-cytokeratins (AE1/AE3) and the epithelial marker Ber-EP4. The detection rate of oncogenenic alterations in LN was significantly higher in RAS-mutant tumors than EGFR mutant tumors (36.36% verse 7.41%, p = 0.017). Patients with oncogenic alterations in LN showed inferior disease-free survival (DFS, p = 0.025) and overall survival (OS, p = 0.027). Furthermore, patients with RAS-mutations detected in LN had the worst DFS and OS (p = 0.001). Among the 11 patients with RAS mutation in primary tumors, DFS and OS in the four patients with mutations detected in LN were significantly shorter than the remaining seven patients without mutations LN (DFS, p = 0.001, OS, p = 0.002). Conclusions: Genomic analysis has the potential to detect oncogenic alterations in regional LNs for localized LUAD and presence of oncogenic alterations in regional LN may be associated with inferior clinical outcome of stage I LUAD, particularly for certain molecular subgroups. ClinicalTrials.gov ID NCT04266691.
Keywords: genomic analysis; lymph node; oncogenic alteration; prognosis; stage I lung adenocarcinoma.
Conflict of interest statement
The molecular detection kit used in this study was sponsored by Amoy Diagnostics Co., Ltd. (AmoyDx). J.Z. is a consultant for Geneplus-Beijing Institute, AstraZeneca and receives research funding and personal fees from Merck, Johnson and Johnson, Roche, OrigiMed, Innovent and Bristol-Myers Squibb outside of the submitted work.
Figures


References
-
- Benlloch S., Galbis-Caravajal J.M., Alenda C., Peiro F.M., Sanchez-Ronco M., Rodriguez-Paniagua J.M., Baschwitz B., Rojas E., Massuti B. Expression of molecular markers in mediastinal nodes from resected stage I non-small-cell lung cancer (NSCLC): Prognostic impact and potential role as markers of occult micrometastases. Ann. Oncol. 2009;20:91–97. doi: 10.1093/annonc/mdn538. - DOI - PubMed
-
- Howington J.A., Blum M.G., Chang A.C., Balekian A.A., Murthy S.C. Treatment of Stage I and II Non-Small Cell Lung Cancer: Diagnosis and Management of Lung Cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e278S–e313S. doi: 10.1378/chest.12-2359. - DOI - PubMed
-
- Martin L.W., D–Cunha J., Wang X., Herzan D., Gu L., Abraham N., Demmy T.L., Detterbeck F.C., Groth S.S., Harpole D.H., et al. Detection of Occult Micrometastases in Patients with Clinical Stage I Non-Small-Cell Lung Cancer: A Prospective Analysis of Mature Results of CALGB 9761 (Alliance) J. Clin. Oncol. 2016;34:1484–1491. doi: 10.1200/JCO.2015.63.4543. - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
