

Interconnections between Inflammageing and Immunosenescence during Ageing
- PMID: 35159168
- PMCID: PMC8834134
- DOI: 10.3390/cells11030359
Interconnections between Inflammageing and Immunosenescence during Ageing
Abstract
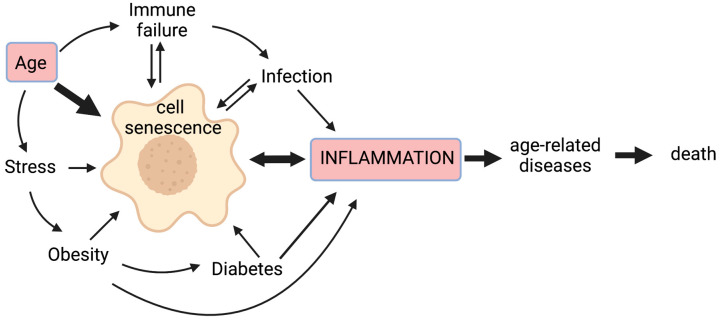
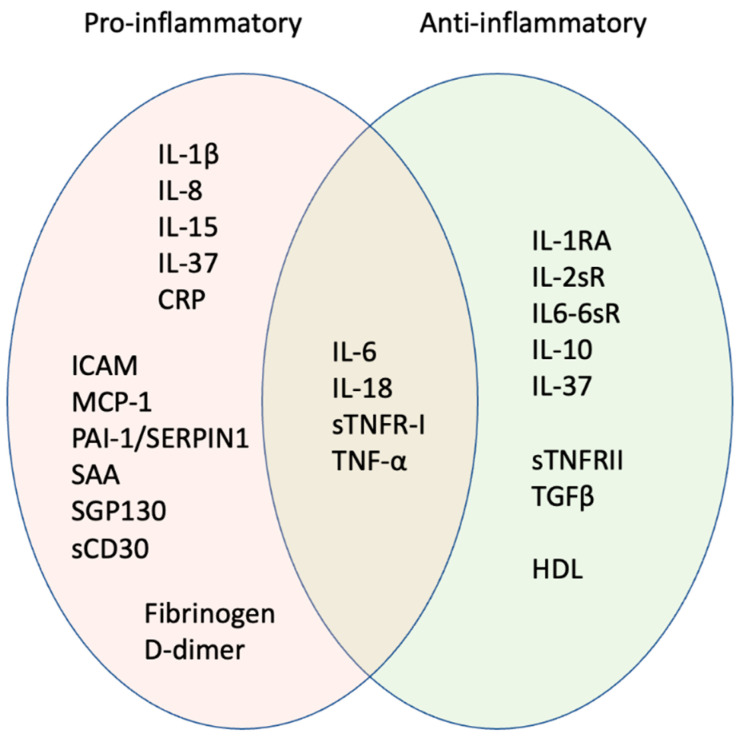
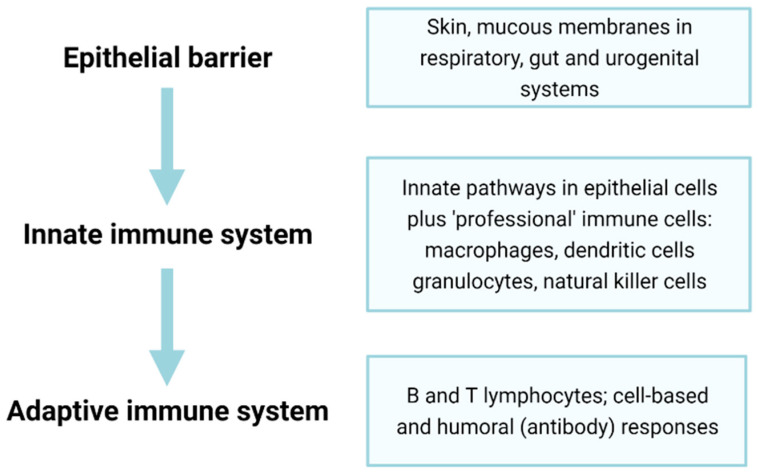
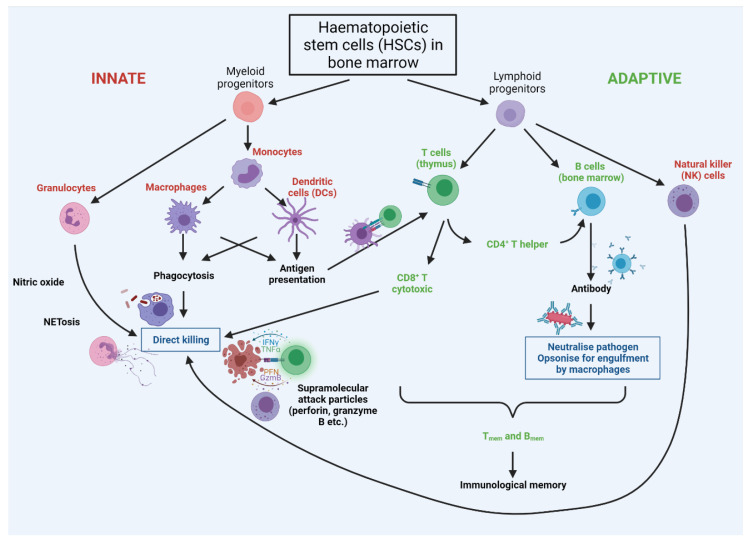
Acute inflammation is a physiological response to injury or infection, with a cascade of steps that ultimately lead to the recruitment of immune cells to clear invading pathogens and heal wounds. However, chronic inflammation arising from the continued presence of the initial trigger, or the dysfunction of signalling and/or effector pathways, is harmful to health. While successful ageing in older adults, including centenarians, is associated with low levels of inflammation, elevated inflammation increases the risk of poor health and death. Hence inflammation has been described as one of seven pillars of ageing. Age-associated sterile, chronic, and low-grade inflammation is commonly termed inflammageing-it is not simply a consequence of increasing chronological age, but is also a marker of biological ageing, multimorbidity, and mortality risk. While inflammageing was initially thought to be caused by "continuous antigenic load and stress", reports from the last two decades describe a much more complex phenomenon also involving cellular senescence and the ageing of the immune system. In this review, we explore some of the main sources and consequences of inflammageing in the context of immunosenescence and highlight potential interventions. In particular, we assess the contribution of cellular senescence to age-associated inflammation, identify patterns of pro- and anti-inflammatory markers characteristic of inflammageing, describe alterations in the ageing immune system that lead to elevated inflammation, and finally assess the ways that diet, exercise, and pharmacological interventions can reduce inflammageing and thus, improve later life health.
Keywords: SASP; ageing; cytokines; immunosenescence; immunosurveillance; inflammageing; inflammation; senescence.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Arai Y., Martin-Ruiz C.M., Takayama M., Abe Y., Takebayashi T., Koyasu S., Suematsu M., Hirose N., von Zglinicki T. Inflammation, But Not Telomere Length, Predicts Successful Ageing at Extreme Old Age: A Longitudinal Study of Semi-Supercentenarians. EBioMedicine. 2015;2:1549–1558. doi: 10.1016/j.ebiom.2015.07.029. - DOI - PMC - PubMed
-
- Bruunsgaard H. The Clinical Impact of Systemic Low-Level Inflammation in Elderly Populations. With Special Reference to Cardiovascular Disease, Dementia and Mortality. Dan. Med. Bull. 2006;53:285–309. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
