

Therapeutic Targeting of Intestinal Fibrosis in Crohn's Disease
- PMID: 35159238
- PMCID: PMC8834168
- DOI: 10.3390/cells11030429
Therapeutic Targeting of Intestinal Fibrosis in Crohn's Disease
Abstract
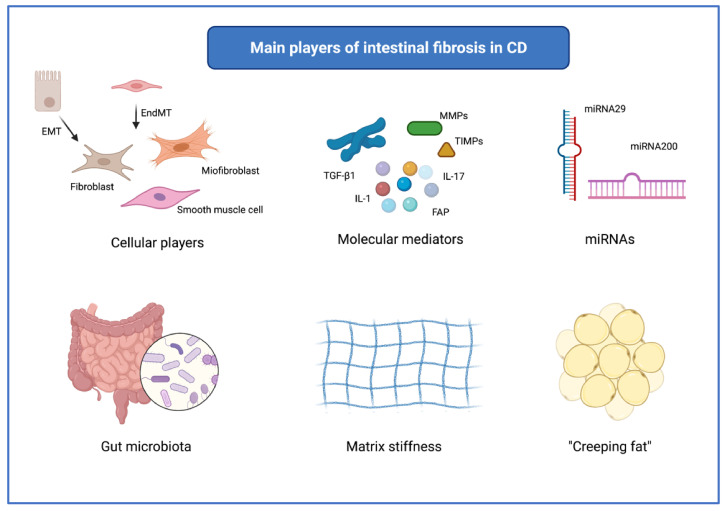
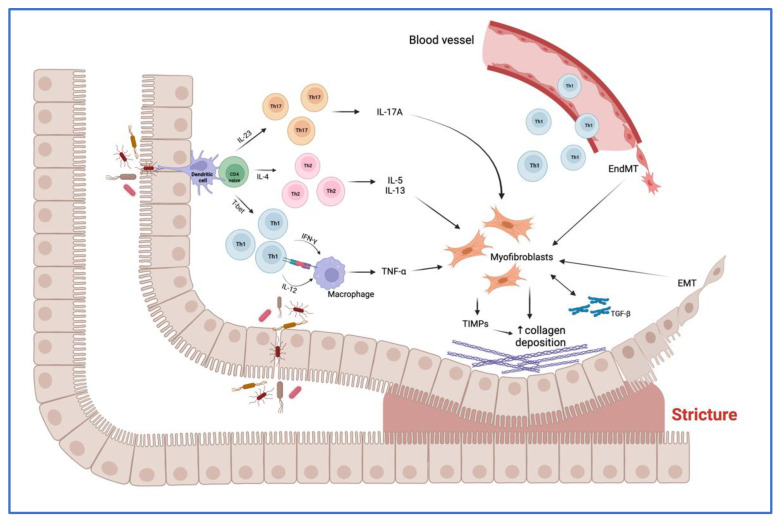
Intestinal fibrosis is one of the most threatening complications of Crohn's disease. It occurs in more than a third of patients with this condition, is associated with increased morbidity and mortality, and surgery often represents the only available therapeutic option. The mechanisms underlying intestinal fibrosis are partly known. Studies conducted so far have shown a relevant pathogenetic role played by mesenchymal cells (especially myofibroblasts), cytokines (e.g., transforming growth factor-β), growth factors, microRNAs, intestinal microbiome, matrix stiffness, and mesenteric adipocytes. Further studies are still necessary to elucidate all the mechanisms involved in intestinal fibrosis, so that targeted therapies can be developed. Although several pre-clinical studies have been conducted so far, no anti-fibrotic therapy is yet available to prevent or reverse intestinal fibrosis. The aim of this review is to provide an overview of the main therapeutic targets currently identified and the most promising anti-fibrotic therapies, which may be available in the near future.
Keywords: Crohn’s disease; IBD; antifibrotic therapy; intestinal fibrosis; stricture.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
