

The Pivotal Role of the Placenta in Normal and Pathological Pregnancies: A Focus on Preeclampsia, Fetal Growth Restriction, and Maternal Chronic Venous Disease
- PMID: 35159377
- PMCID: PMC8833914
- DOI: 10.3390/cells11030568
The Pivotal Role of the Placenta in Normal and Pathological Pregnancies: A Focus on Preeclampsia, Fetal Growth Restriction, and Maternal Chronic Venous Disease
Abstract
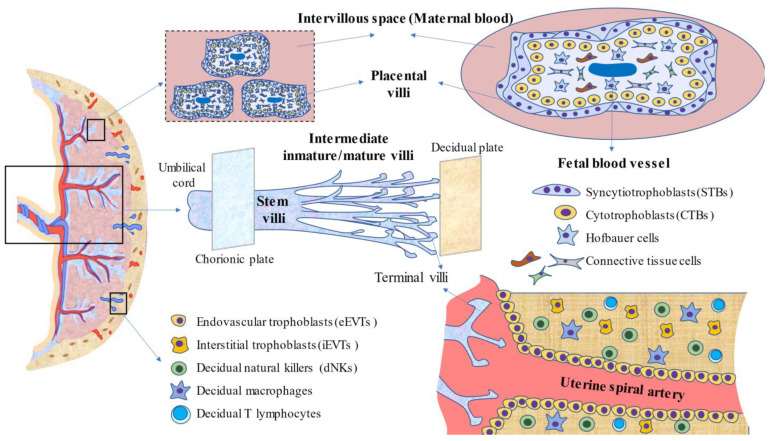
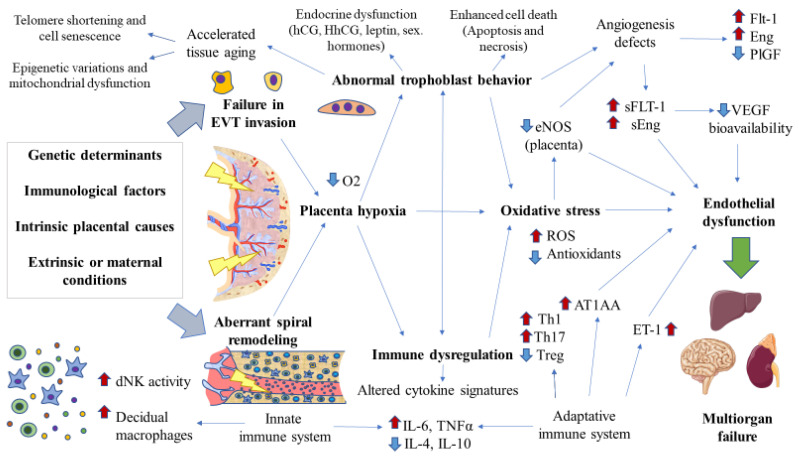
The placenta is a central structure in pregnancy and has pleiotropic functions. This organ grows incredibly rapidly during this period, acting as a mastermind behind different fetal and maternal processes. The relevance of the placenta extends far beyond the pregnancy, being crucial for fetal programming before birth. Having integrative knowledge of this maternofetal structure helps significantly in understanding the development of pregnancy either in a proper or pathophysiological context. Thus, the aim of this review is to summarize the main features of the placenta, with a special focus on its early development, cytoarchitecture, immunology, and functions in non-pathological conditions. In contraposition, the role of the placenta is examined in preeclampsia, a worrisome hypertensive disorder of pregnancy, in order to describe the pathophysiological implications of the placenta in this disease. Likewise, dysfunction of the placenta in fetal growth restriction, a major consequence of preeclampsia, is also discussed, emphasizing the potential clinical strategies derived. Finally, the emerging role of the placenta in maternal chronic venous disease either as a causative agent or as a consequence of the disease is equally treated.
Keywords: fetal growth restriction; maternal chronic venous disease (CVeD); placenta; preeclampsia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
