

3D Echo Characterization of Proportionate and Disproportionate Functional Mitral Regurgitation before and after Percutaneous Mitral Valve Repair
- PMID: 35160100
- PMCID: PMC8836818
- DOI: 10.3390/jcm11030645
3D Echo Characterization of Proportionate and Disproportionate Functional Mitral Regurgitation before and after Percutaneous Mitral Valve Repair
Abstract
Background: The impact of percutaneous mitral valve repair (PMVr) on long-term prognosis in patients with functional mitral regurgitation (FMR) is still unclear. Recently, a new conceptual framework classifying FMR as proportionate (P-MR) and disproportionate (D-MR) was proposed, according to the effective regurgitant orifice area/left ventricular end-diastolic volume (EROA/LVEDV) ratio. The aim was to assess its possible influence on PMVr efficacy.
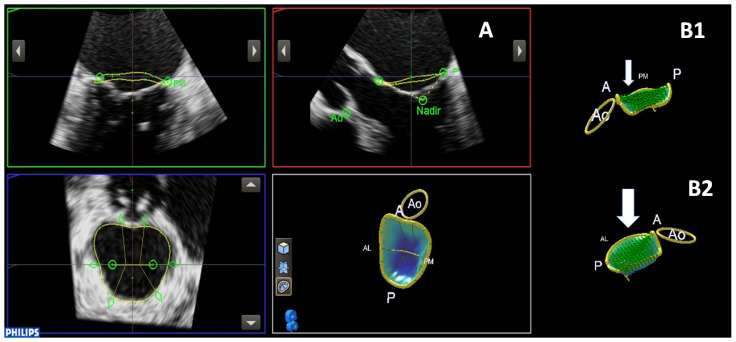
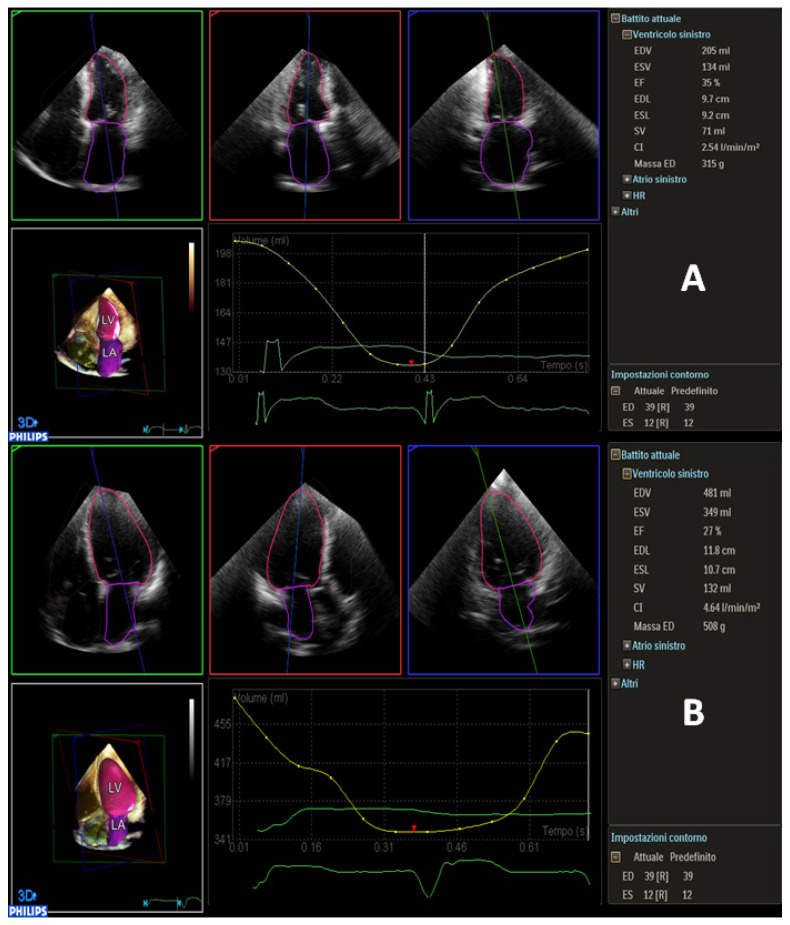
Methods: A total of 56 patients were enrolled. MV annulus, LV volumes and function were assessed. Global longitudinal strain (GLS) was also calculated. Patients were divided into two groups, according to the EROA/LVEDV ratio. Echocardiographic follow-up was performed after 6 months, and adverse events were collected after 12 months.
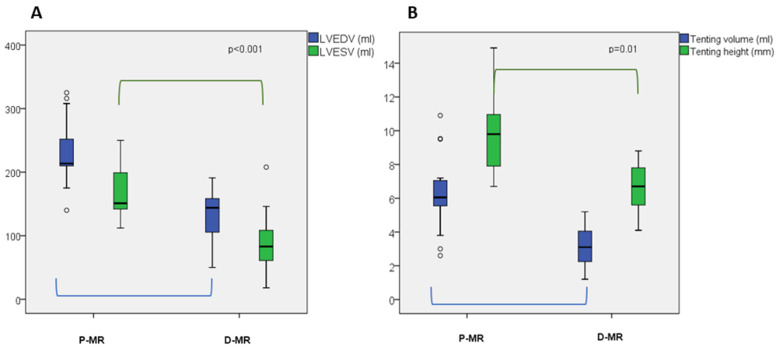
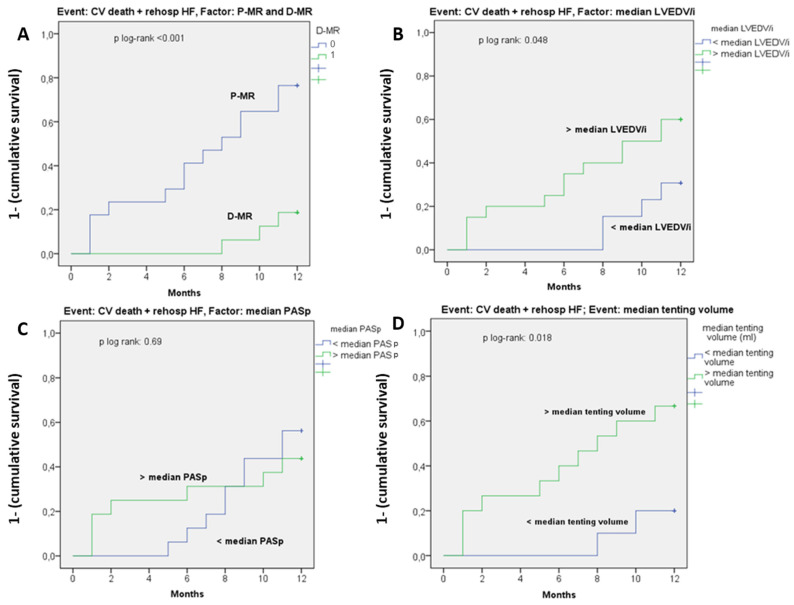
Results: D-MR patients (n = 28, 50%) had a significantly more elliptical MV annulus (p = 0.048), lower tenting volume (p = 0.01), higher LV ejection fraction (LVEF: 32 ± 7 vs. 26 ± 5%, p = 0.003), lower LVEDV, LV end-systolic volume (LVESV) and mass (LVEDV/i: 80 ± 20 vs. 126 ± 27 mL, p = 0.001; LVESV/i: 60 ± 20 vs. 94 ± 23 mL, p < 0.001; LV mass: 249 ± 63 vs. 301 ± 69 gr, p = 0.035). GLS was more impaired in P-MR (p = 0.048). After 6 months, P-MR patients showed a higher rate of MR recurrence. After 12 months, the rate of CV death and rehospitalization due to HF was significantly higher in P-MR patients (46% vs. 7%, p < 0.001). P-MR status was strongly associated with CV death/rehospitalization (HR = 3.4, CI 95% = 1.3-8.6, p = 0.009).
Conclusions: Patients with P-MR seem to have worse outcomes after PVMr than D-MR patients. Our study confirms the importance of the EROA/LVEDV ratio in defining different subsets of FMR based on the anatomical characteristic of MV and LV.
Keywords: EROA/LVEDV ratio; MitraClip; PMVr; disproportionate MR; functional mitral regurgitation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ponikowski P., Voors A.A., Anker S.D., Bueno H., Cleland J.G.F., Coats A.J.S., Falk V., González-Juanatey J.R., Harjola V.-P., Jankowska E.A., et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016;18:891–975. doi: 10.1002/ejhf.592. - DOI - PubMed
-
- Stone G.W., Vahanian A.S., Adams D.H., Abraham W.T., Borer J.S., Bax J.J., Schofer J., Cutlip D.E., Krucoff M.W., Blackstone E.H., et al. Clinical Trial Design Principles and Endpoint Definitions for Transcatheter Mitral Valve Repair and Replacement: Part 1: Clinical Trial Design Principles. J. Am. Coll. Cardiol. 2015;66:278–307. doi: 10.1016/j.jacc.2015.05.046. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
