

Magnetic Resonance for Differential Diagnosis of Left Ventricular Hypertrophy: Diagnostic and Prognostic Implications
- PMID: 35160102
- PMCID: PMC8836982
- DOI: 10.3390/jcm11030651
Magnetic Resonance for Differential Diagnosis of Left Ventricular Hypertrophy: Diagnostic and Prognostic Implications
Abstract
Background: Left ventricular hypertrophy (LVH) may be due to different causes, ranging from benign secondary forms to severe cardiomyopathies. Transthoracic Echocardiography (TTE) and ECG are the first-level examinations for LVH diagnosis. Cardiac magnetic resonance (CMR) accurately defines LVH type, extent and severity.
Objectives: to evaluate the diagnostic and prognostic role of CMR in patients with TTE and/or ECG evidence of LVH.
Methods: We performed CMR in 300 consecutive patients with echocardiographic and/or ECG signs of LVH.
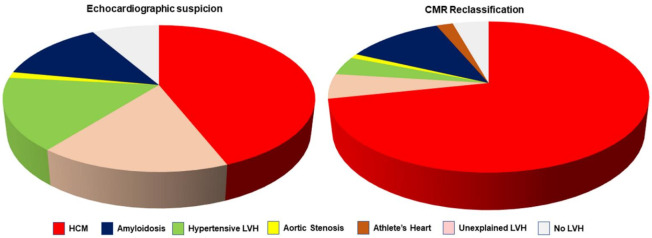
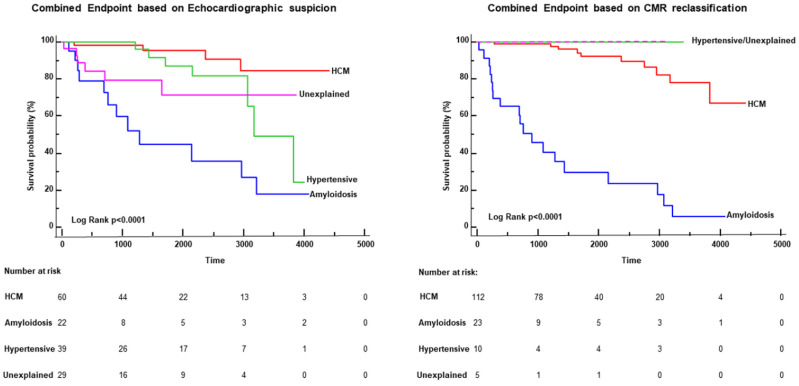
Results: Overall, 275 patients had TTE evidence of LVH, with initial suspicion of hypertrophic cardiomyopathy (HCM) in 132 (44%), cardiac amyloidosis in 41 (14%), hypertensive LVH in 48 (16%), aortic stenosis in 4 (1%), and undetermined LVH in 50 (16%). The initial echocardiographic diagnostic suspicion of LVH was confirmed in 172 patients (57.3%) and changed in 128 patients (42.7%, p < 0.0001): the diagnosis of HCM increased from 44% to 71% of patients; hypertensive and undetermined LVH decreased significantly (respectively to 4% and 5%). CMR allowed for a diagnosis in 41 out of 50 (82%) patients with undetermined LVH at TTE. CMR also identified HCM in 17 out of 25 patients with apparently normal echocardiography but with ECG criteria for LVH. Finally, the reclassification of the diagnosis by CMR was associated with a change in survival risk of patients: after CMR reclassification, no events occurred in patients with undetermined or hypertensive LVH.
Conclusions: CMR changed echocardiographic suspicion in almost half of patients with LVH. In the subgroup of patients with abnormal ECG, CMR identified LVH (particularly HCM) in 80% of patients. This study highlights the indication of CMR to better characterize the type, extent and severity of LVH detected at echocardiography and suspected with ECG.
Keywords: echocardiography; left ventricular hypertrophy; magnetic resonance; prognosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Elliott P.M., Anastasakis A., Borger M.A., Borggrefe M., Cecchi F., Charron P., Hagege A.A., Lafont A., Limongelli G., Mahrholdt H., et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC) Eur. Heart J. 2014;35:2733–2779. - PubMed
LinkOut - more resources
Full Text Sources
