

Lymphopenia as a Predictor for Adverse Clinical Outcomes in Hospitalized Patients with COVID-19: A Single Center Retrospective Study of 4485 Cases
- PMID: 35160150
- PMCID: PMC8837002
- DOI: 10.3390/jcm11030700
Lymphopenia as a Predictor for Adverse Clinical Outcomes in Hospitalized Patients with COVID-19: A Single Center Retrospective Study of 4485 Cases
Abstract
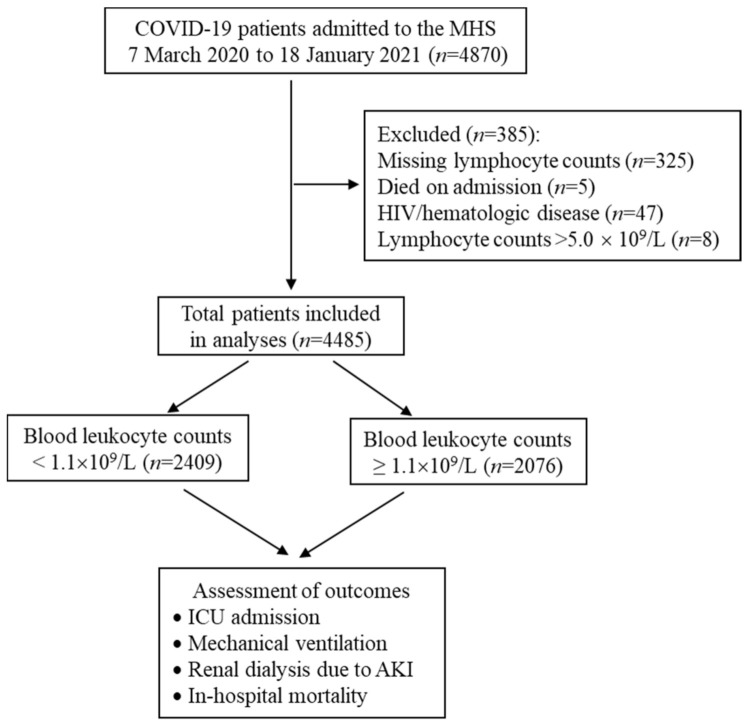
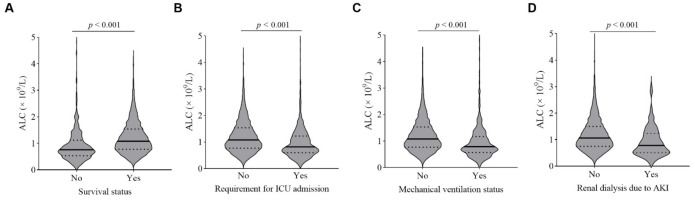
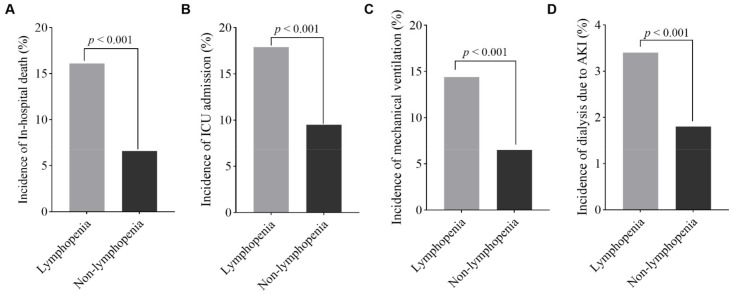
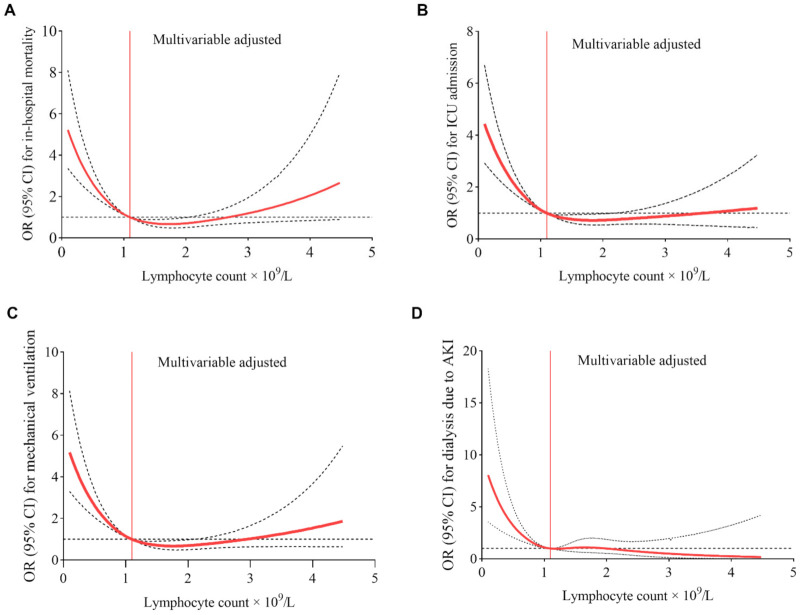
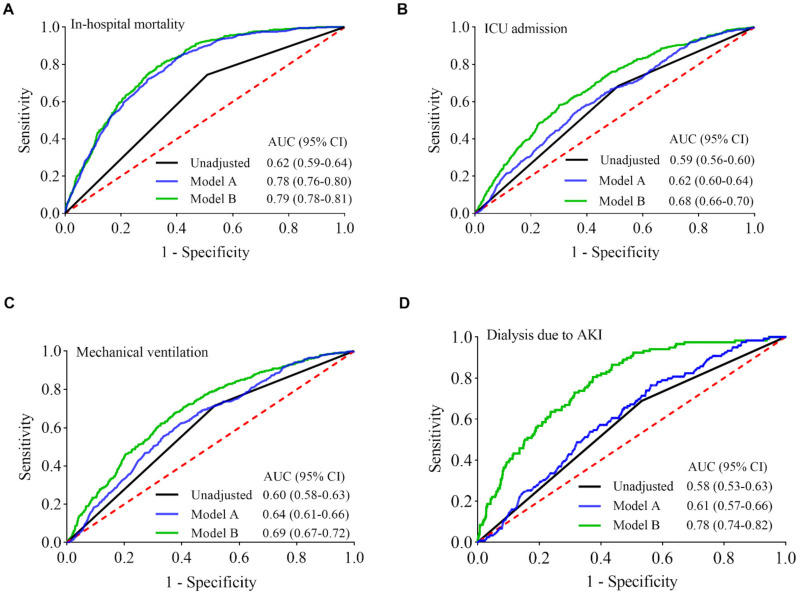
Lymphopenia is commonly present in patients with COVID-19. We sought to determine if lymphopenia on admission predicts COVID-19 clinical outcomes. A retrospective chart review was performed on 4485 patients with laboratory-confirmed COVID-19, who were admitted to the hospital. Of those, 2409 (57.3%) patients presented with lymphopenia (absolute lymphocyte count < 1.1 × 109/L) on admission, and had higher incidences of ICU admission (17.9% versus 9.5%, p < 0.001), invasive mechanical ventilation (14.4% versus 6.5%, p < 0.001), dialysis (3.4% versus 1.8%, p < 0.001) and in-hospital mortality (16.6% versus 6.6%, p < 0.001), with multivariable-adjusted odds ratios of 1.86 (95% confidence interval [CI], 1.55-2.25), 2.09 (95% CI, 1.69-2.59), 1.77 (95% CI, 1.19-2.68), and 2.19 (95% CI 1.76-2.72) for the corresponding outcomes, respectively, compared to those without lymphopenia. The restricted cubic spline models showed a non-linear relationship between lymphocyte count and adverse outcomes, with an increase in the risk of adverse outcomes for lower lymphocyte counts in patients with lymphopenia. The predictive powers of lymphopenia, expressed as areas under the receiver operating characteristic curves, were 0.68, 0.69, 0.78, and 0.79 for the corresponding adverse outcomes, respectively, after incorporating age, gender, race, and comorbidities. In conclusion, lymphopenia is a useful metric in prognosticating outcomes in hospitalized COVID-19 patients.
Keywords: COVID-19; adverse clinical outcomes; lymphocyte count; lymphopenia; receiver operating characteristic curves; restricted cubic splines.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Biolè C., Bianco M., Núñez-Gil I.J., Cerrato E., Spirito A., Roubin S.R., Viana-Llamas M.C., Gonzalez A., Castro-Mejía A.F., Eid C.M., et al. Gender Differences in the Presentation and Outcomes of Hospitalized Patients With COVID-19. J. Hosp. Med. 2021;16:349–352. doi: 10.12788/jhm.3594. - DOI - PubMed
-
- Núñez-Gil I.J., Fernández-Pérez C., Estrada V., Becerra-Muñoz V.M., El-Battrawy I., Uribarri A., Fernández-Rozas I., Feltes G., Viana-Llamas M.C., Trabattoni D., et al. Mortality risk assessment in Spain and Italy, insights of the HOPE COVID-19 registry. Intern. Emerg. Med. 2020;16:957–966. doi: 10.1007/s11739-020-02543-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
