

Ankle Magnetic Resonance Imaging in Juvenile Idiopathic Arthritis Versus Non-Juvenile Idiopathic Arthritis Patients with Arthralgia
- PMID: 35160212
- PMCID: PMC8837053
- DOI: 10.3390/jcm11030760
Ankle Magnetic Resonance Imaging in Juvenile Idiopathic Arthritis Versus Non-Juvenile Idiopathic Arthritis Patients with Arthralgia
Abstract
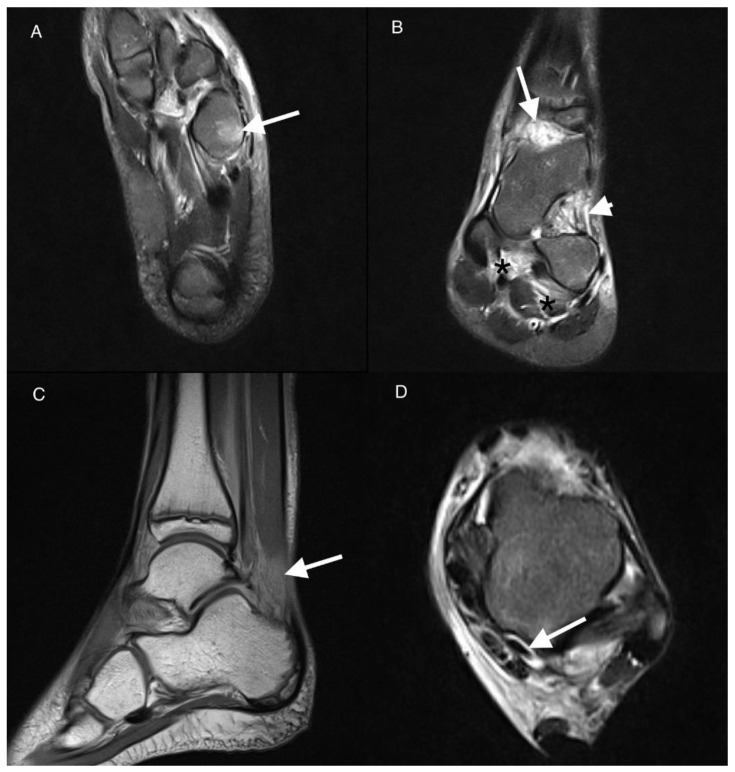
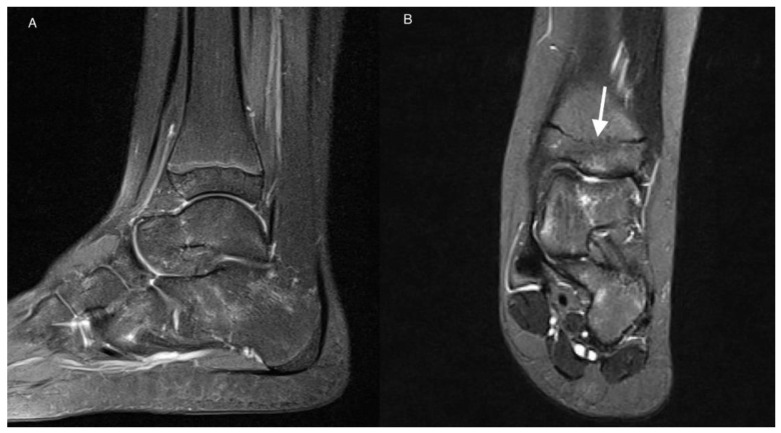
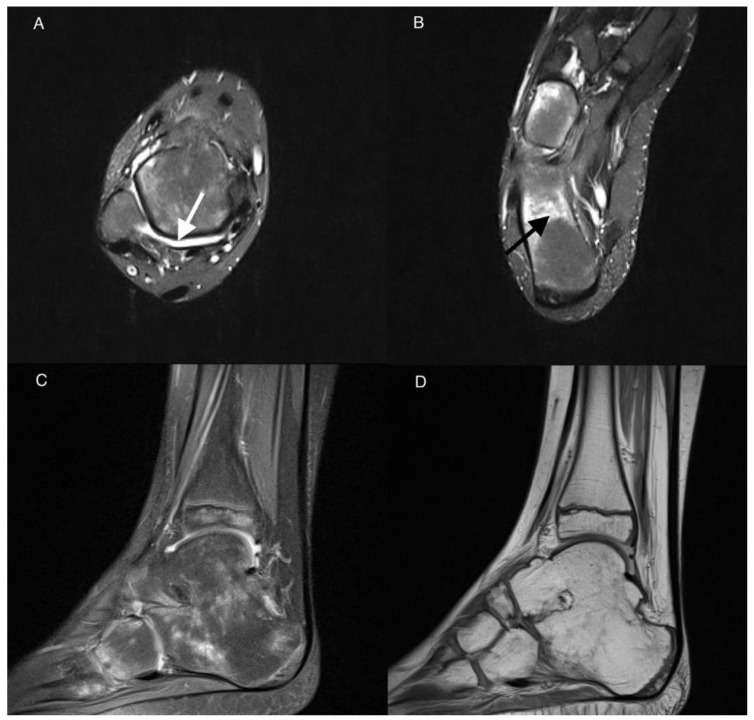
This retrospective case-control study aimed to evaluate whether Magnetic Resonance Imaging (MRI) enables differentiation of ankle arthritis in Juvenile Idiopathic Afrthritis JIA from ankle arthralgia of unknown aetiology in patients clinically suspected of JIA. Forty-four children, at ages 5-16, who underwent MRI of the ankle from January 2016 to March 2021 for clinically suspected active ankle arthritis in the course of JIA were included. MRI findings in both groups-patients with the final diagnosis of JIA and without final diagnosis of JIA-were compared and scored. The sum of the scores of 22 ankle lesions in an individual patient (active, destructive and developmental), so-called the MRI summarized score, was calculated and tested in terms of the most optimal diagnosis of JIA. Interobserver agreement was calculated. Inflammatory features were seen on MRI in 38 out of all the included patients (86%). The most common lesions in both groups were effusion in the tibio-talar joint (68% in JIA and 64% in the arthralgia group) and effusion in subtalar joint (64% in JIA vs. 59% in the arthralgia group). In general, more lesions were identified in the JIA group than in non-JIA. However, only tenosynovitis was significantly more common in the JIA vs. non-JIA group (p = 0.031). The MRI summarized score did not allow for discrimination between ankle arthritis in JIA from non-JIA patients; the best levels of sensitivity (32%), specificity (91%), positive predictive value PPV (78%) and negative predictive value NPV (57%) were achieved only at the cut-off point of 10.
Keywords: ankle arthritis; juvenile idiopathic arthritis; magnetic resonance imaging; scoring.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Lovell D.J. Juvenile idiopathic arthritis: Clinical features. In: Klippel J.H., Stone J.H., Crofford L.J., White P.F., editors. Primer on the Rheumatic Diseases. Springer; New York, NY, USA: 2008. pp. 142–148.
LinkOut - more resources
Full Text Sources
