

Postural Control Differences between Patients with Posterior Tibial Tendon Dysfunction and Healthy People during Gait
- PMID: 35162324
- PMCID: PMC8835140
- DOI: 10.3390/ijerph19031301
Postural Control Differences between Patients with Posterior Tibial Tendon Dysfunction and Healthy People during Gait
Abstract
Background: Patients with posterior tibial tendon dysfunction (PTTD) may exhibit postural instability during walking likely due to a loss of medial longitudinal arch, abnormal foot alignment, and pain. While many studies have investigated gait alterations in PTTD, there is no understanding of dynamic postural control mechanisms in this population during gait, which will help guide rehabilitation and gait training programs for patients with PTTD. The purpose of the study was to assess dynamic postural control mechanisms in patients with stage II PTTD as compared to age and gender matched healthy controls.
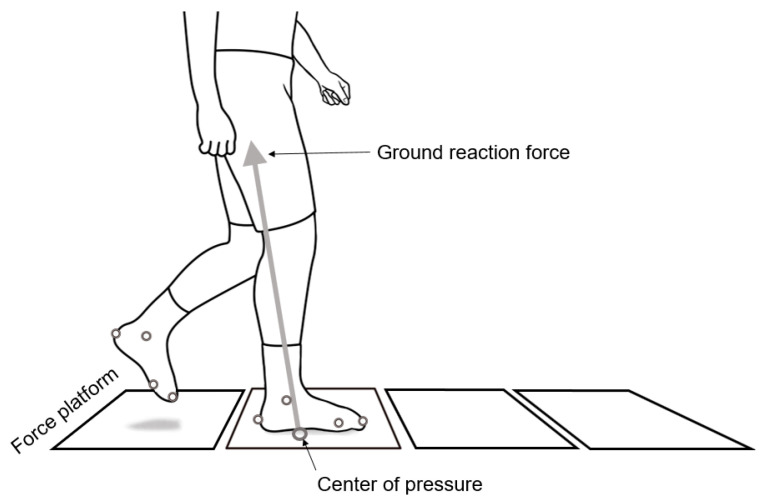
Methods: Eleven patients with stage II PTTD (4 males and 7 females; age 59 ± 1 years; height 1.66 ± 0.12 m; mass 84.2 ± 16.0 kg) and ten gender and age matched controls were recruited in this study. Participants were asked to walk along a 10 m walkway. Ten Vicon cameras and four AMTI force platforms were used to collect kinematic and center of pressure (COP) data while participants performed gait. To test differences between PTTD vs. control groups, independent t-tests (set at α < 0.05) were performed.
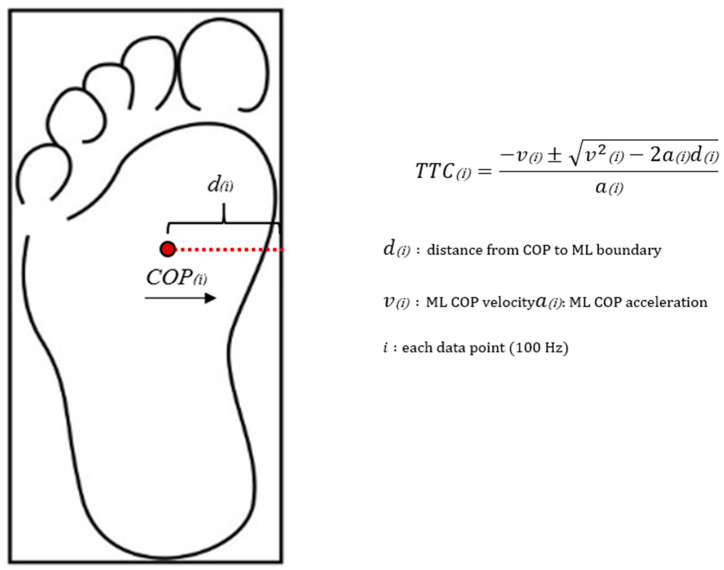
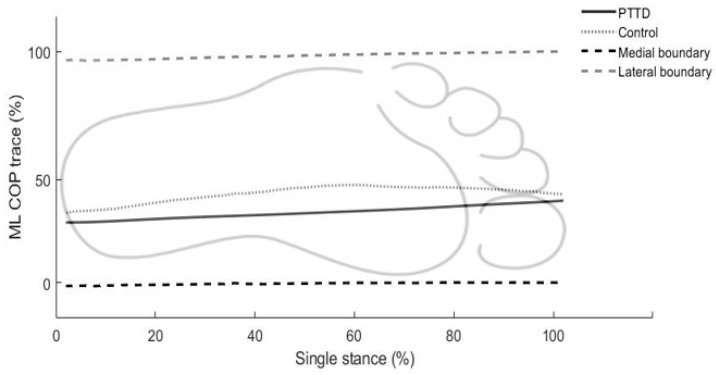
Results: Patients with PTTD had significantly higher double stance ratio (+23%) and anterior-posterior (AP) time to contact (TTC) percentage (+16%) as compared to healthy control. However, PTTD had lower AP COP excursion (-19%), AP COP velocity (-30%), and medial-lateral (ML) COP velocity (-40%) as compared to healthy controls. Mean ML COP trace values for PTTD were significantly decreased (-23%) as compared to controls, indicating COP trace for PTTD tends to be closer to the medial boundary than controls during single-support phase of walking.
Conclusion: PTTD patients showed more conservative and cautious postural strategies which may help maintain balance and reduce the need for postural adjustment during PTTD gait. They also showed more medially shifted COP patterns than healthy controls during single-support phase of walking. Dynamic postural control outcomes could be used to develop effective gait training programs aimed at alleviating a medial shift of COP (everted foot) for individuals with PTTD in order to improve their functionality and gait efficiency.
Keywords: PTTD; center of pressure; gait; postural control; time-to-boundary.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Comparison of changes in posterior tibialis muscle length between subjects with posterior tibial tendon dysfunction and healthy controls during walking.J Orthop Sports Phys Ther. 2007 Nov;37(11):661-9. doi: 10.2519/jospt.2007.2539. J Orthop Sports Phys Ther. 2007. PMID: 18057670
-
Comparison of foot kinematics between subjects with posterior tibialis tendon dysfunction and healthy controls.J Orthop Sports Phys Ther. 2006 Sep;36(9):635-44. doi: 10.2519/jospt.2006.2293. J Orthop Sports Phys Ther. 2006. PMID: 17017268
-
A kinematic and kinetic analysis of the hip and knee joints in patients with posterior tibialis tendon dysfunction; comparison with healthy age-matched controls.Gait Posture. 2018 Oct;66:228-235. doi: 10.1016/j.gaitpost.2018.08.040. Epub 2018 Sep 5. Gait Posture. 2018. PMID: 30212782
-
Gait alterations in posterior tibial tendonitis: A systematic review and meta-analysis.Gait Posture. 2020 Feb;76:28-38. doi: 10.1016/j.gaitpost.2019.11.002. Epub 2019 Nov 4. Gait Posture. 2020. PMID: 31715431
-
Self-reported social and activity restrictions accompany local impairments in posterior tibial tendon dysfunction: a systematic review.J Foot Ankle Res. 2018 Aug 30;11:49. doi: 10.1186/s13047-018-0292-z. eCollection 2018. J Foot Ankle Res. 2018. PMID: 30186369 Free PMC article.
Cited by
-
Effects of arch support doses on the center of pressure and pressure distribution of running using statistical parametric mapping.Front Bioeng Biotechnol. 2022 Nov 21;10:1051747. doi: 10.3389/fbioe.2022.1051747. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36479433 Free PMC article.
References
-
- Myerson M.S. Adult acquired flatfoot deformity: Treatment of dysfunction of the posterior tibial tendon. Instr. Course Lect. 1997;46:393–405. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
