

Therapeutic Strategies for Disseminated Intravascular Coagulation Associated with Aortic Aneurysm
- PMID: 35163216
- PMCID: PMC8836167
- DOI: 10.3390/ijms23031296
Therapeutic Strategies for Disseminated Intravascular Coagulation Associated with Aortic Aneurysm
Abstract
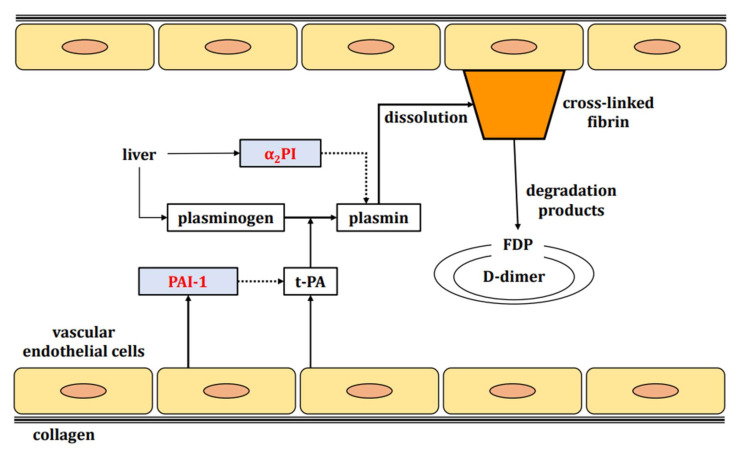
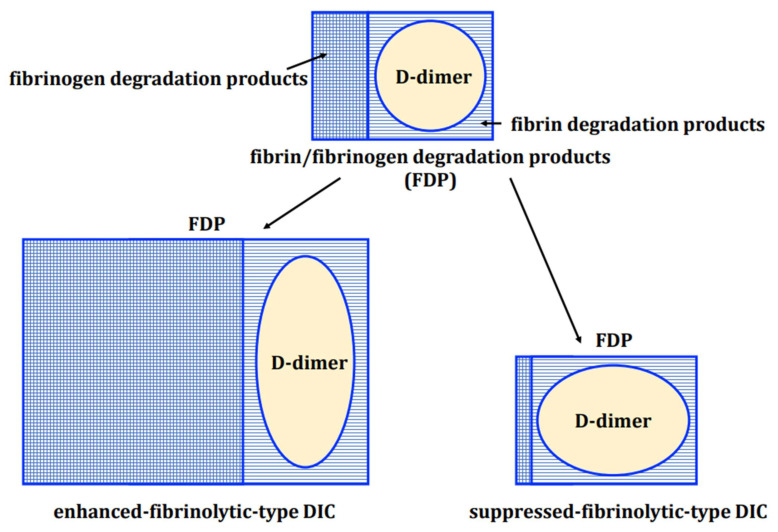
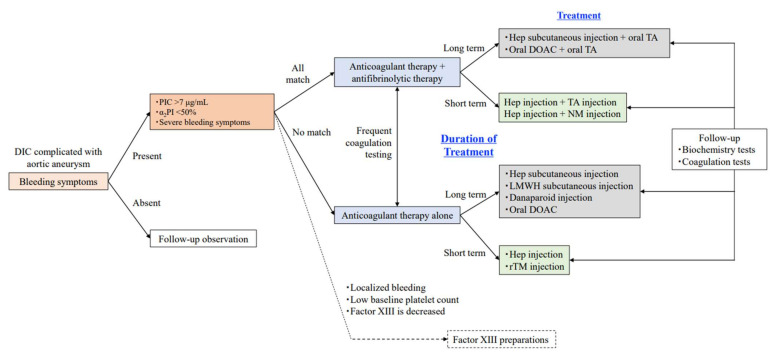
Aortic aneurysms are sometimes associated with enhanced-fibrinolytic-type disseminated intravascular coagulation (DIC). In enhanced-fibrinolytic-type DIC, both coagulation and fibrinolysis are markedly activated. Typical cases show decreased platelet counts and fibrinogen levels, increased concentrations of fibrin/fibrinogen degradation products (FDP) and D-dimer, and increased FDP/D-dimer ratios. Thrombin-antithrombin complex or prothrombin fragment 1 + 2, as markers of coagulation activation, and plasmin-α2 plasmin inhibitor complex, a marker of fibrinolytic activation, are all markedly increased. Prolongation of prothrombin time (PT) is not so obvious, and the activated partial thromboplastin time (APTT) is rather shortened in some cases. As a result, DIC can be neither diagnosed nor excluded based on PT and APTT alone. Many of the factors involved in coagulation and fibrinolysis activation are serine proteases. Treatment of enhanced-fibrinolytic-type DIC requires consideration of how to control the function of these serine proteases. The cornerstone of DIC treatment is treatment of the underlying pathology. However, in some cases surgery is either not possible or exacerbates the DIC associated with aortic aneurysm. In such cases, pharmacotherapy becomes even more important. Unfractionated heparin, other heparins, synthetic protease inhibitors, recombinant thrombomodulin, and direct oral anticoagulants (DOACs) are agents that inhibit serine proteases, and all are effective against DIC. Inhibition of activated coagulation factors by anticoagulants is key to the treatment of DIC. Among them, DOACs can be taken orally and is useful for outpatient treatment. Combination therapy of heparin and nafamostat allows fine-adjustment of anticoagulant and antifibrinolytic effects. While warfarin is an anticoagulant, this agent is ineffective in the treatment of DIC because it inhibits the production of coagulation factors as substrates without inhibiting activated coagulation factors. In addition, monotherapy using tranexamic acid in cases of enhanced-fibrinolytic-type DIC may induce fatal thrombosis. If tranexamic acid is needed for DIC, combination with anticoagulant therapy is of critical importance.
Keywords: direct oral anticoagulant; enhanced-fibrinolytic-type disseminated intravascular coagulation; nafamostat; serine protease; synthetic protease inhibitor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Mukaiyama H., Shinoyama S., Ikezawa T., Kamiya T., Hamaguchi M., Saito H. Abdominal aortic aneurysm complicated with chronic disseminated intravascular abdominal aortic aneurysm with chronic disseminated intravascular coagulopathy: A case of surgical treatment. J. Vasc. Surg. 1987;6:600–604. doi: 10.1016/0741-5214(87)90278-3. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
