

Therapeutic Treatments for Osteoporosis-Which Combination of Pills Is the Best among the Bad?
- PMID: 35163315
- PMCID: PMC8836178
- DOI: 10.3390/ijms23031393
Therapeutic Treatments for Osteoporosis-Which Combination of Pills Is the Best among the Bad?
Abstract
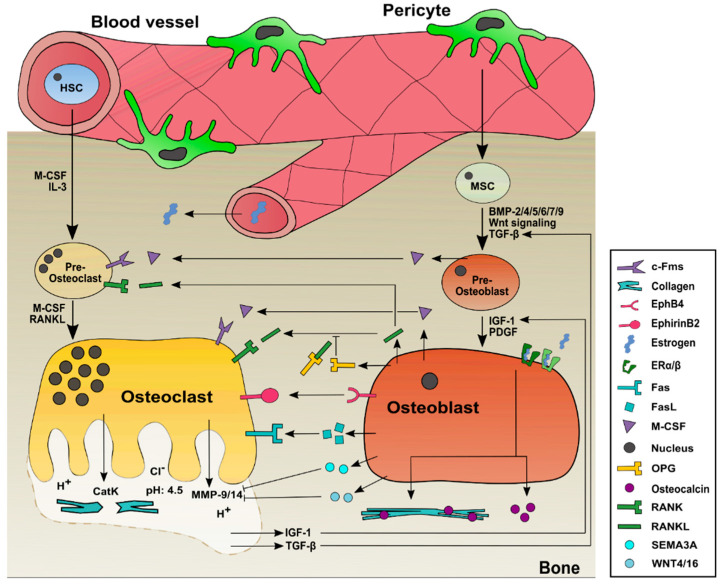
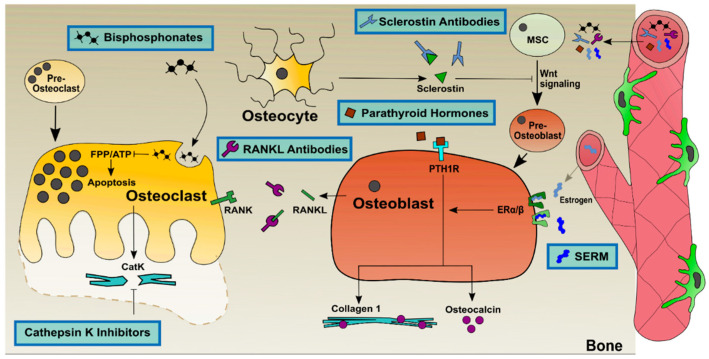
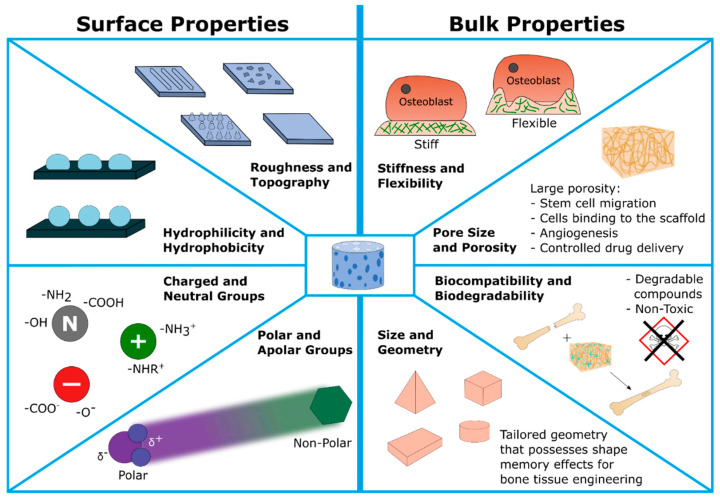
Osteoporosis is a chronical, systemic skeletal disorder characterized by an increase in bone resorption, which leads to reduced bone density. The reduction in bone mineral density and therefore low bone mass results in an increased risk of fractures. Osteoporosis is caused by an imbalance in the normally strictly regulated bone homeostasis. This imbalance is caused by overactive bone-resorbing osteoclasts, while bone-synthesizing osteoblasts do not compensate for this. In this review, the mechanism is presented, underlined by in vitro and animal models to investigate this imbalance as well as the current status of clinical trials. Furthermore, new therapeutic strategies for osteoporosis are presented, such as anabolic treatments and catabolic treatments and treatments using biomaterials and biomolecules. Another focus is on new combination therapies with multiple drugs which are currently considered more beneficial for the treatment of osteoporosis than monotherapies. Taken together, this review starts with an overview and ends with the newest approaches for osteoporosis therapies and a future perspective not presented so far.
Keywords: anabolic; biomaterial; bone mineral density; bone remodeling; catabolic; combination of treatments; osteoblast; osteoclast; osteoporosis; treatment.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
Osteoporosis: From Molecular Mechanisms to Therapies.Int J Mol Sci. 2020 Jan 22;21(3):714. doi: 10.3390/ijms21030714. Int J Mol Sci. 2020. PMID: 31979046 Free PMC article.
-
Current and emerging bone resorption inhibitors for the treatment of osteoporosis.Expert Opin Pharmacother. 2025 Feb;26(3):265-278. doi: 10.1080/14656566.2025.2451741. Epub 2025 Jan 15. Expert Opin Pharmacother. 2025. PMID: 39797385 Review.
-
Perspectives on osteoporosis therapies.J Endocrinol Invest. 2015 Mar;38(3):303-11. doi: 10.1007/s40618-014-0236-9. Epub 2015 Jan 11. J Endocrinol Invest. 2015. PMID: 25577263 Review.
-
Osteoblast-n-Osteoclast: Making Headway to Osteoporosis Treatment.Curr Drug Targets. 2020;21(16):1640-1651. doi: 10.2174/1389450121666200731173522. Curr Drug Targets. 2020. PMID: 32735518 Review.
-
Osteoporosis: now and the future.Lancet. 2011 Apr 9;377(9773):1276-87. doi: 10.1016/S0140-6736(10)62349-5. Epub 2011 Mar 28. Lancet. 2011. PMID: 21450337 Free PMC article. Review.
Cited by
-
The beneficial effects of simultaneous supplementation of Lactobacillus reuteri and calcium fluoride nanoparticles on ovariectomy-induced osteoporosis.BMC Complement Med Ther. 2023 Sep 26;23(1):340. doi: 10.1186/s12906-023-04167-6. BMC Complement Med Ther. 2023. PMID: 37752485 Free PMC article.
-
Characteristics and osteogenic mechanism of glycosylated peptides-calcium chelate.Curr Res Food Sci. 2022 Oct 17;5:1965-1975. doi: 10.1016/j.crfs.2022.10.008. eCollection 2022. Curr Res Food Sci. 2022. PMID: 36312881 Free PMC article.
-
Pro-differentiative, Pro-adhesive and Pro-migratory Activities of Isorhamnetin in MC3T3-E1 Osteoblasts via Activation of ERK-dependent BMP2-Smad Signaling.Cell Biochem Biophys. 2024 Dec;82(4):3607-3617. doi: 10.1007/s12013-024-01450-2. Epub 2024 Aug 13. Cell Biochem Biophys. 2024. PMID: 39136840
-
Wnt/β-catenin signaling pathway: proteins' roles in osteoporosis and cancer diseases and the regulatory effects of natural compounds on osteoporosis.Mol Med. 2024 Oct 28;30(1):193. doi: 10.1186/s10020-024-00957-x. Mol Med. 2024. PMID: 39468464 Free PMC article. Review.
-
17β-Estradiol-Loaded Exosomes for Targeted Drug Delivery in Osteoporosis: A Comparative Study of Two Loading Methods.Adv Pharm Bull. 2023 Nov;13(4):736-746. doi: 10.34172/apb.2023.072. Epub 2023 Feb 1. Adv Pharm Bull. 2023. PMID: 38022800 Free PMC article.
References
-
- Burr D.B. Basic and Applied Bone Biology. Elsevier; Cambridge, MA, USA: 2019. Bone morphology and organization; pp. 3–26.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
