

The Physiology of Insulin Clearance
- PMID: 35163746
- PMCID: PMC8836929
- DOI: 10.3390/ijms23031826
The Physiology of Insulin Clearance
Abstract
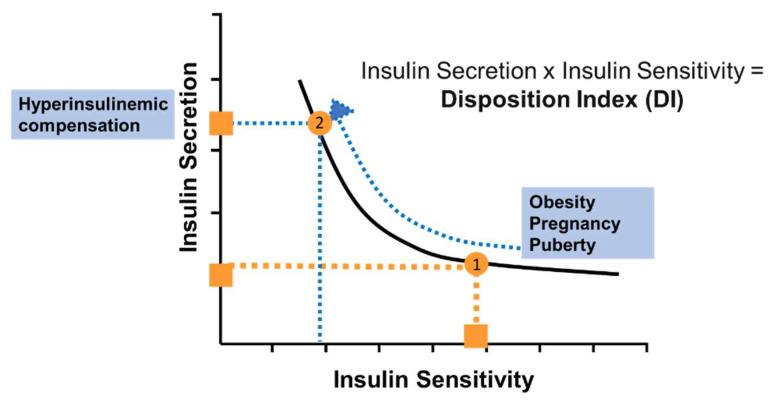
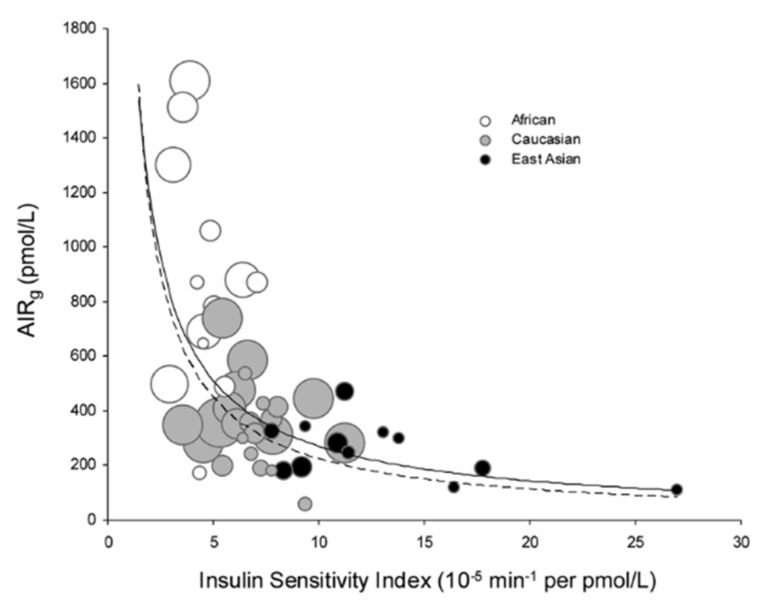
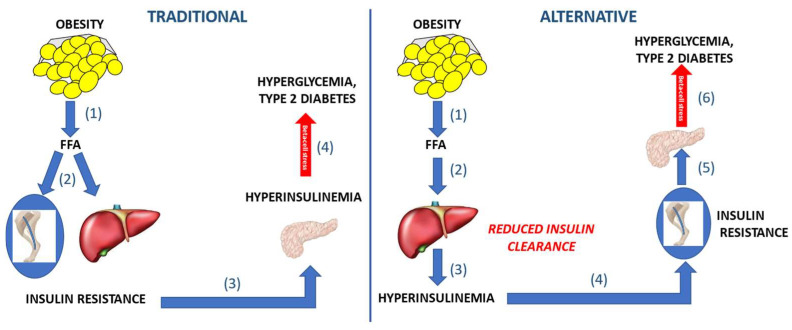
In the 1950's, Dr. I. Arthur Mirsky first recognized the possible importance of insulin degradation changes to the pathogenesis of type 2 diabetes. While this mechanism was ignored for decades, insulin degradation is now being recognized as a possible factor in diabetes risk. After Mirsky, the relative importance of defects in insulin release and insulin resistance were recognized as risk factors. The hyperbolic relationship between secretion and sensitivity was introduced, as was the relationship between them, as expressed as the disposition index (DI). The DI was shown to be affected by environmental and genetic factors, and it was shown to be differentiated among ethnic groups. However, the importance of differences in insulin degradation (clearance) on the disposition index relationship remains to be clarified. Direct measure of insulin clearance revealed it to be highly variable among even normal individuals, and to be affected by fat feeding and other physiologic factors. Insulin clearance is relatively lower in ethnic groups at high risk for diabetes such as African Americans and Hispanic Americans, compared to European Americans. These differences exist even for young children. Two possible mechanisms have been proposed for the importance of insulin clearance for diabetes risk: in one concept, insulin resistance per se leads to reduced clearance and diabetes risk. In a second and new concept, reduced degradation is a primary factor leading to diabetes risk, such that lower clearance (resulting from genetics or environment) leads to systemic hyperinsulinemia, insulin resistance, and beta-cell stress. Recent data by Chang and colleagues appear to support this latter hypothesis in Native Americans. The importance of insulin clearance as a risk factor for metabolic disease is becoming recognized and may be treatable.
Keywords: beta-cell failure; disposition index; insulin clearance; type 2 diabetes.
Conflict of interest statement
The authors declare no conflict of interest relevant to this article.
Figures
References
-
- National Institutes of Health Clinical Guidelines on the Identification, Evaluation; Treatment of Overweight and Obesity in Adults—The Evidence Report. Obes. Res. 1998;6((Suppl. S2)):51s–209s. - PubMed
-
- Mirsky I.A., Broh-Kahn R.H. The inactivation of insulin by tissue extracts; the distribution and properties of insulin inactivating extracts. Arch. Biochem. 1949;20:1–9. - PubMed
-
- Simkin B., Broh-Kahn R.H., Mirsky I.A. The inactivation of insulin by tissue extracts; the effect of force-fed diets on the insulinase activity of rat liver extracts. Arch. Biochem. 1949;24:422–428. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
