

Passive leg raising in brain injury patients within the neurointensive care unit. A prospective trial
- PMID: 35164482
- PMCID: PMC10158487
- DOI: 10.5114/ait.2021.108361
Passive leg raising in brain injury patients within the neurointensive care unit. A prospective trial
Abstract
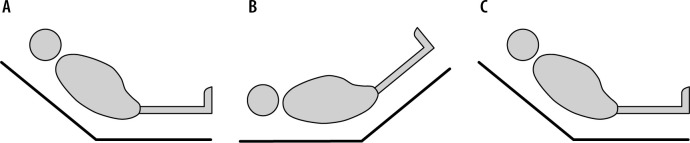
Introduction: In critically ill brain-injured patients maintaining balanced fluid management is a crucial part of critical care. Many factors influence the relationship between fluid management, cerebral blood flow and cerebral oxygenation. Passive leg raising (PLR)-induced changes predict fluid responsiveness in the majority of non-neurological ICU patients. In patients with intracranial lesions, PLR testing has been hypothesized to increase intracranial pressure (ICP), although data are lacking. We wanted to investigate the feasibility of PLR with expected intracranial pressure increase, according to the higher cerebral blood volume. This should be self-limiting in patients with intact cerebral autoregulation.
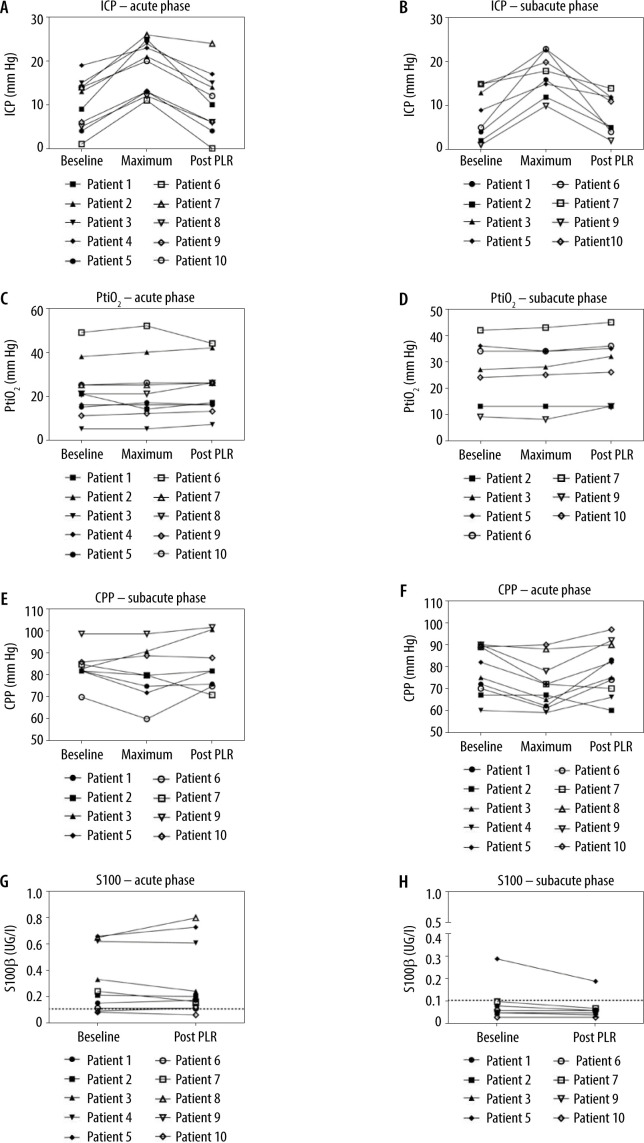
Material and methods: We prospectively included patients with traumatic brain injury (TBI) or aneurysmal subarachnoid hemorrhage (aSAH) in this pilot trial. PLR was performed within 48 hours after the initial diagnosis and on days 5-8. All patients had ICP monitoring. Absence of intracranial hypertension (defined as ICP < 25 mm Hg) was considered a positive test result.
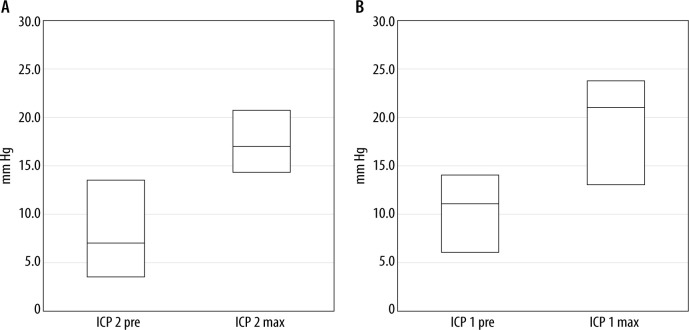
Results: Ten patients were recruited for this study. The cohort consisted of 6 male patients with TBI and 4 female patients with aSAH. Mean patient age was 55.6 years (range 35-76). Overall, 18 tests could be performed, of which only one had to be terminated due to temporarily elevated ICP. 9 out of 10 patients had no intracranial hypertension during the acute (mean ICP increase 8.45 mm Hg, range 4-16) or during the subacute phase (mean ICP increase 9.12 mm Hg, range 3-18).
Conclusions: PLR is feasible in patients with intracranial pathology to assess fluid responsiveness and provide optimized patient volume management without increasing the risk of persistent intracranial hypertension.
Keywords: fluid administration; intracranial hypertension; neurointensive care.; passive leg raise; subarachnoid hemorrhage; traumatic brain injury.
Conflict of interest statement
none.
Figures
References
-
- Le Roux P, Menon DK, Citerio G, et al. Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care: a statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Intensive Care Med 2014; 40: 1189-1209. doi: 10.1007/s00134-014-3369-6. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources