

Glottic views using a Miller size 0 blade are superior to those from a Macintosh size 0 blade in neonates: a randomized trial
- PMID: 35164484
- PMCID: PMC10165327
- DOI: 10.5114/ait.2021.108561
Glottic views using a Miller size 0 blade are superior to those from a Macintosh size 0 blade in neonates: a randomized trial
Abstract
Introduction: Both the Miller and Macintosh blades are commonly used during laryngoscopy in infants and children, although the glottic views have not been compared in neonates. This study compared the glottic views with the Miller and Macintosh size 0 blades in neonates when the blades were placed above and below the epiglottis.
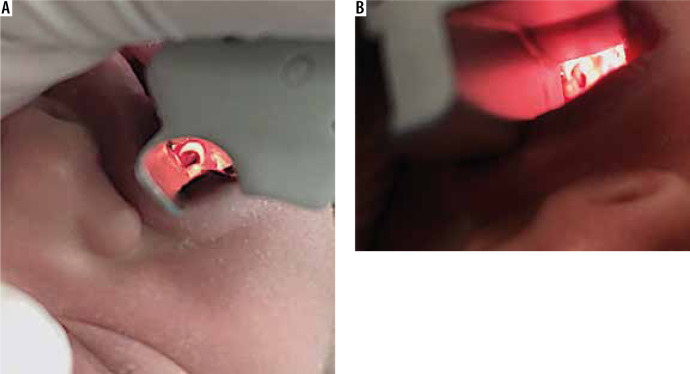
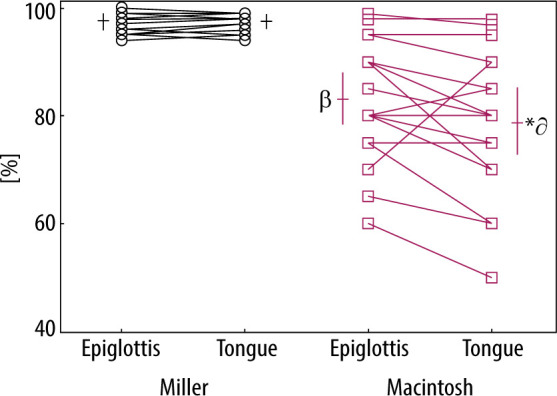
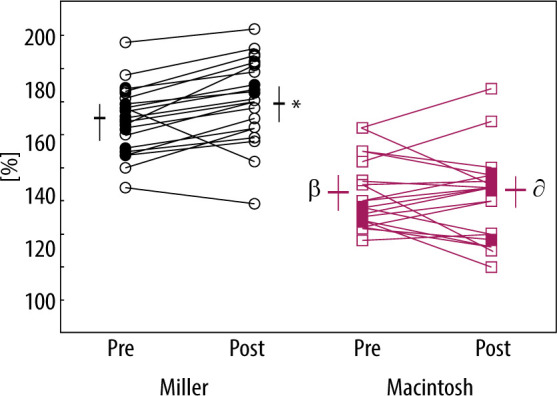
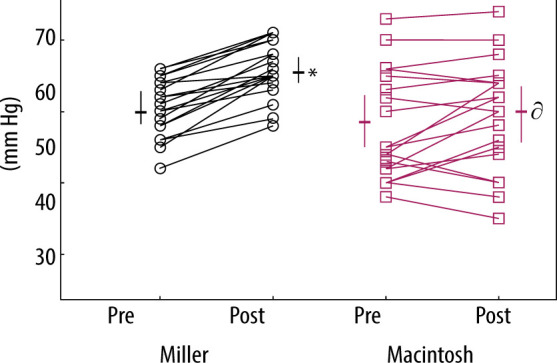
Material and methods: Forty anaesthetized and paralyzed neonates undergoing elective surgery were enrolled and randomized to either the Miller or Macintosh size 0 blade. Two glottic views were obtained in random order in each neonate and were photographed using the same blade: lifting the epiglottis first then the tongue base or vice versa. The percentage of glottic opening (POGO) scores were evaluated with each view. The POGO scores and cardiorespiratory variables were then analysed.
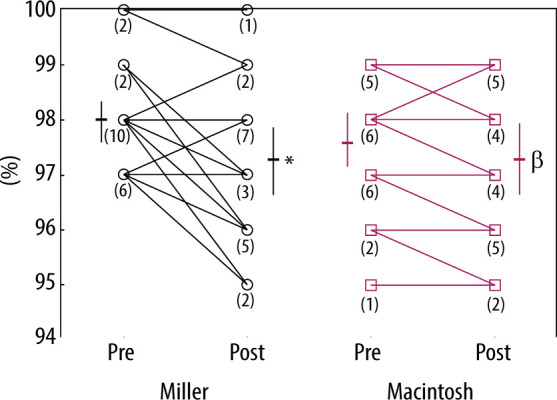
Results: The POGO scores using the Miller blade to lift both the epiglottis and the tongue base were similar, whereas the scores using the Macintosh blade to lift the epiglottis were greater than those to lift the tongue base. The POGO scores using the Miller blade in both positions were significantly greater than those using the Macintosh blade in the corresponding positions (P = 0.0001). The heart rate using the Miller blade was greater than that using the Macintosh blade (P = 0.0001).
Conclusions: In neonates, the glottic views using the Miller size 0 blade to lift both the epiglottis and the tongue base were deemed to be excellent and superior to those using the Macintosh blade in both positions.
Keywords: glottic view.; laryngoscope; laryngoscopy; neonate.
Conflict of interest statement
none.
Figures
References
-
- Passi Y, Sathyamoorthy M, Lerman J, Heard C, Marino M. Comparison of the laryngoscopy views with the size 1 Miller and Macintosh laryngoscope blades lifting the epiglottis or the base of the tongue in infants and children <2 yr of age. Br J Anaesth 2014; 113: 869-874. doi: 10.1093/bja/aeu228. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources