

COVID-19 Pandemic Impact on Percutaneous Coronary Intervention for Acute Coronary Syndromes: An Australian Tertiary Centre Experience
- PMID: 35165052
- PMCID: PMC8836676
- DOI: 10.1016/j.hlc.2021.10.019
COVID-19 Pandemic Impact on Percutaneous Coronary Intervention for Acute Coronary Syndromes: An Australian Tertiary Centre Experience
Abstract
Background: Countries who suffered large COVID-19 outbreaks reported a decrease in acute coronary syndrome (ACS) presentations and percutaneous coronary intervention (PCI). The impact of the pandemic in countries like Australia, with relatively small outbreaks yet significant social restrictions, is relatively unknown. There is also limited and conflicting data regarding the impact on clinical outcomes, symptom-to-door time (STDT) and door-to-balloon time (DTBT).
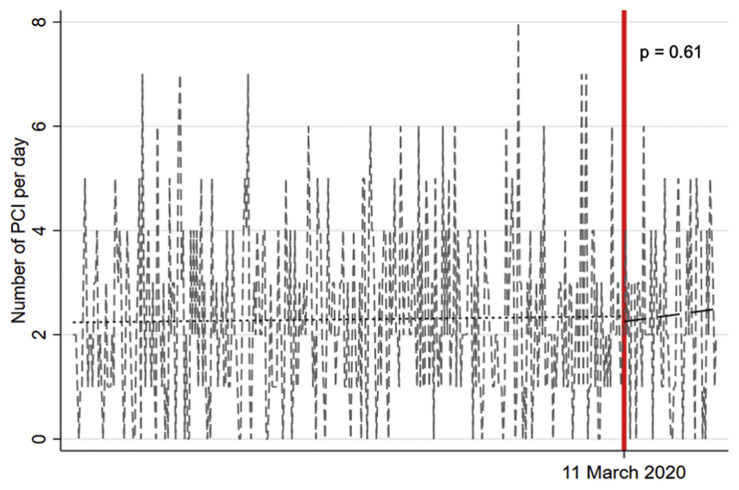
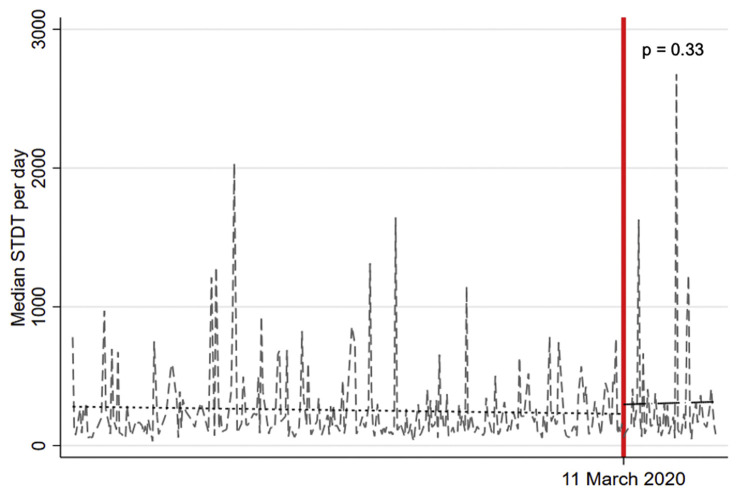
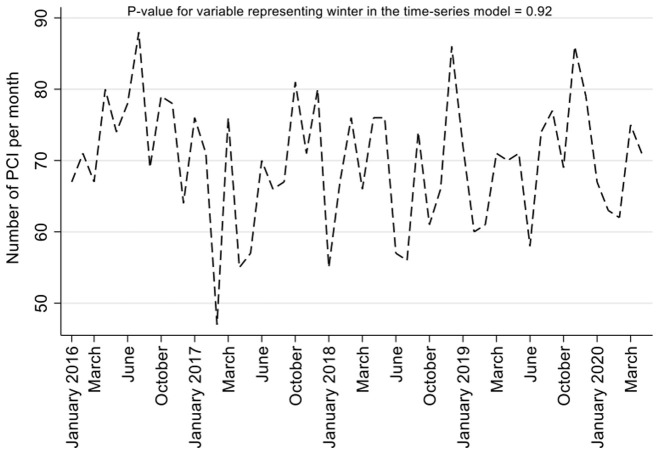
Methods: Consecutive ACS patients treated with PCI were prospectively recruited from a tertiary hospital network in Melbourne, Australia. The pre-pandemic period (11 March 2019-10 March 2020) was compared to the pandemic period (11 March 2020-10 May 2020) using an interrupted time series analysis with a primary endpoint of number PCI-treated ACS per day. Secondary endpoints included STDT, DTBT, total mortality and major adverse cardiac events (MACE).
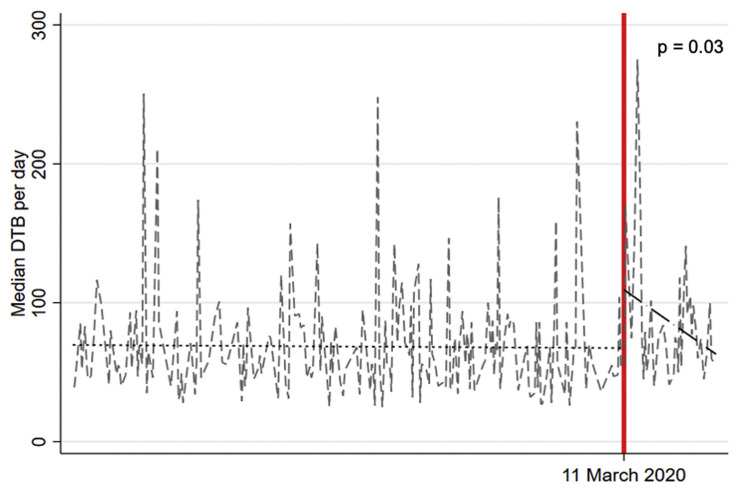
Results: A total 984 ACS patients (14.8% during the pandemic period) received PCI. Mean number of PCI-treated ACS per day did not differ between the two periods (2.3 vs 2.4, p=0.61) with no difference in STDT [+51.3 mins, 95% confidence interval (CI) -52.4 to 154.9, p=0.33], 30-day mortality (5% vs 5.3%, p=0.86) or MACE (5.2% vs 6.1%, p=0.68). DTBT was significantly longer during the pandemic versus the pre-pandemic period (+18.1 mins, 95% CI 1.6-34.5, p=0.03) and improved with time (slope estimate: -0.76, 95% CI -1.62 to 0.10).
Conclusions: Despite significant social restrictions imposed in Melbourne, numbers of ACS treated with PCI and 30-day outcomes were similar to pre-pandemic times. DTBT was significantly longer during the COVID-19 pandemic period, likely reflecting infection control measures, which reassuringly improved with time.
Keywords: Acute coronary syndrome; COVID-19; Pandemic; Percutaneous coronary intervention.
Copyright © 2021 Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS) and the Cardiac Society of Australia and New Zealand (CSANZ). Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Rodríguez-Leor O., Cid-Álvarez B., Ojeda S., Martín-Moreiras J., Rumoroso J.R., López-Palop R., et al. Impact of the COVID-19 pandemic on interventional cardiology activity in Spain. REC Interv Cardiol. 2020
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
