

The Pathogenesis and Long-Term Consequences of COVID-19 Cardiac Injury
- PMID: 35165665
- PMCID: PMC8828362
- DOI: 10.1016/j.jacbts.2021.10.011
The Pathogenesis and Long-Term Consequences of COVID-19 Cardiac Injury
Abstract
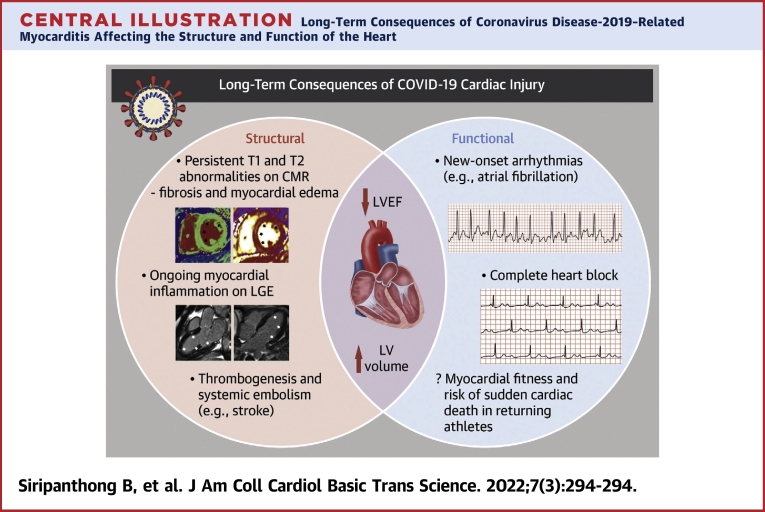
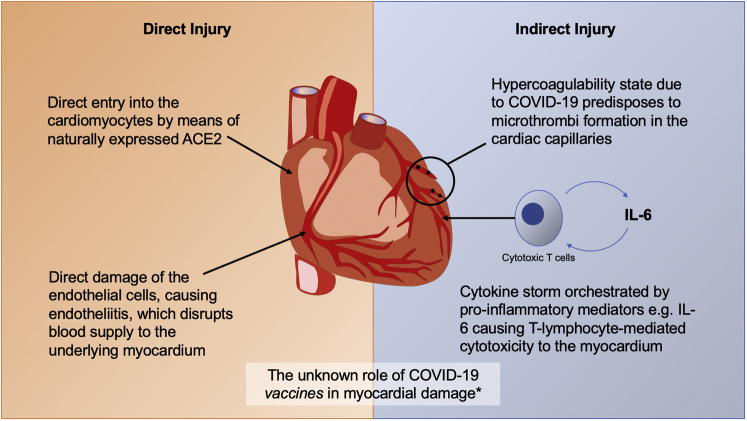
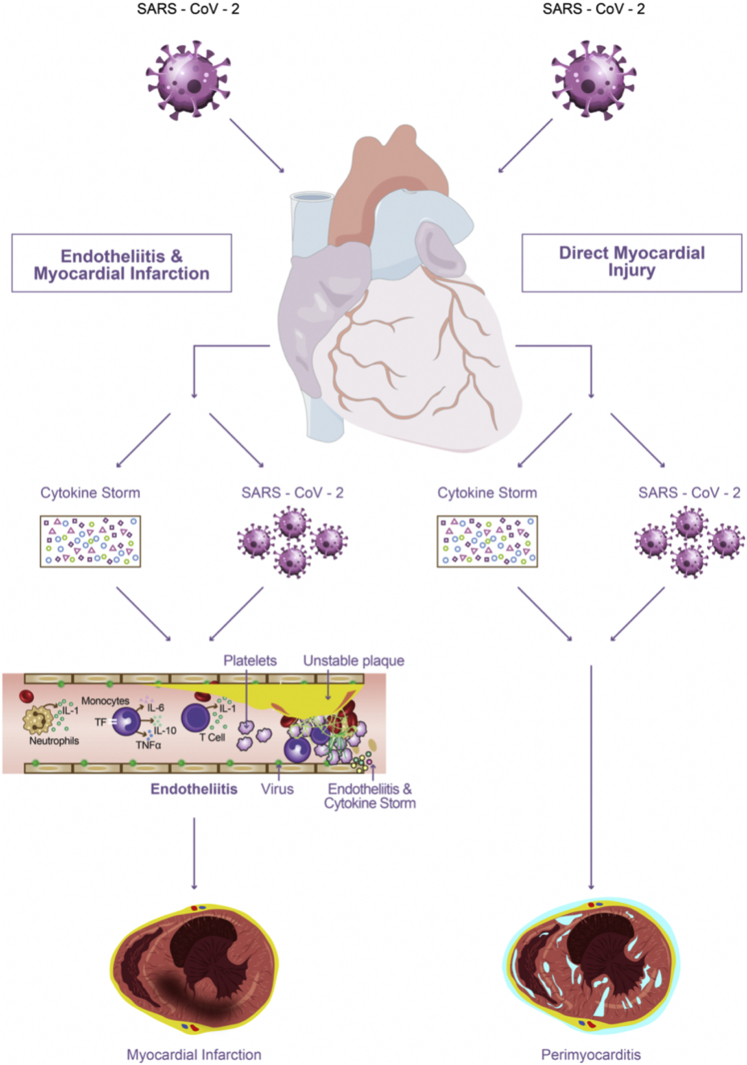
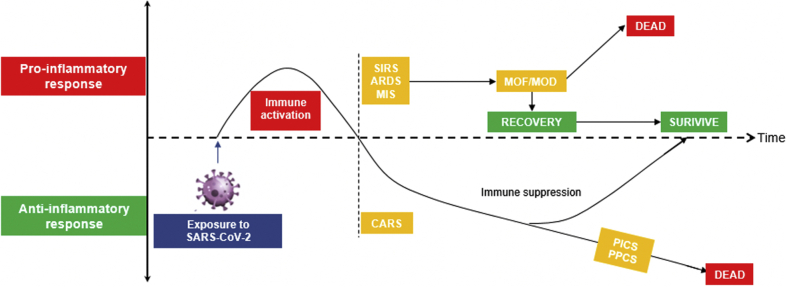
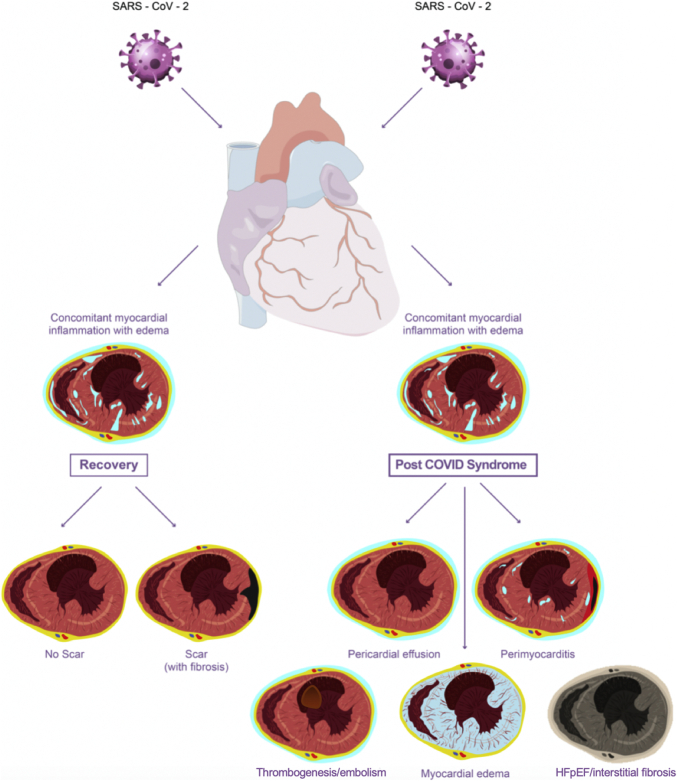
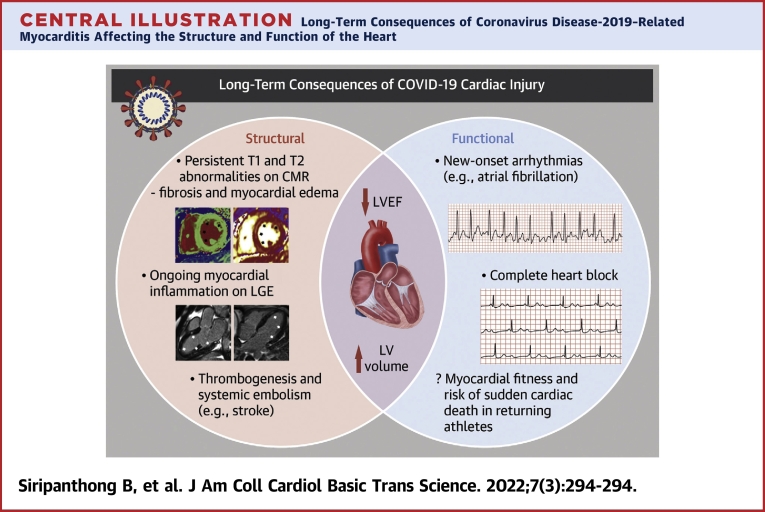
The mechanisms of coronavirus disease-2019 (COVID-19)-related myocardial injury comprise both direct viral invasion and indirect (hypercoagulability and immune-mediated) cellular injuries. Some patients with COVID-19 cardiac involvement have poor clinical outcomes, with preliminary data suggesting long-term structural and functional changes. These include persistent myocardial fibrosis, edema, and intraventricular thrombi with embolic events, while functionally, the left ventricle is enlarged, with a reduced ejection fraction and new-onset arrhythmias reported in a number of patients. Myocarditis post-COVID-19 vaccination is rare but more common among young male patients. Larger studies, including prospective data from biobanks, will be useful in expanding these early findings and determining their validity.
Keywords: CMR, cardiovascular magnetic resonance; COVID-19; COVID-19, coronavirus disease-2019; CT, Computerized Tomography; LGE, late gadolinium enhancement; MI, myocardial infarction; SARS-CoV-2, severe acute respiratory syndrome coronavirus-2; athlete; cardiovascular magnetic resonance imaging; inflammation; myocardial injury; myocarditis; sudden cardiac death; troponin.
© 2022 The Authors.
Conflict of interest statement
Dr Nazarian has received grants from the National Institutes of Health, ImriCor, Biosense Webster, and ADAS; and is a consultant to CardioSolv and ImroCor. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Worldometer COVID-19 pandemic live update. https://www.worldometers.info/coronavirus/ Accessed July 3, 2021.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
