

Predictive ability of severity scores and outcomes for mortality in kidney transplant recipients with coronavirus disease 2019 admitted to the intensive care unit: results from a Brazilian single-center cohort study
- PMID: 35166299
- PMCID: PMC9518629
- DOI: 10.1590/2175-8239-JBN-2021-0155
Predictive ability of severity scores and outcomes for mortality in kidney transplant recipients with coronavirus disease 2019 admitted to the intensive care unit: results from a Brazilian single-center cohort study
Abstract
Background: the predictive ability of severity scores for mortality in patients admitted to intensive care units is not well-known among kidney transplanted (KT) patients, especially those diagnosed with coronavirus disease 2019 (COVID-19). The purpose of the present study was to evaluate the predictive ability of severity scores for mortality in KT recipients.
Methods: 51 KT recipients with COVID-19 diagnosis were enrolled. The performance of the SOFA, SAPS 3, and APACHE IV tools in predicting mortality after COVID-19 was compared by the area under the ROC curve (AUC-ROC) and univariate Cox regression analysis was performed.
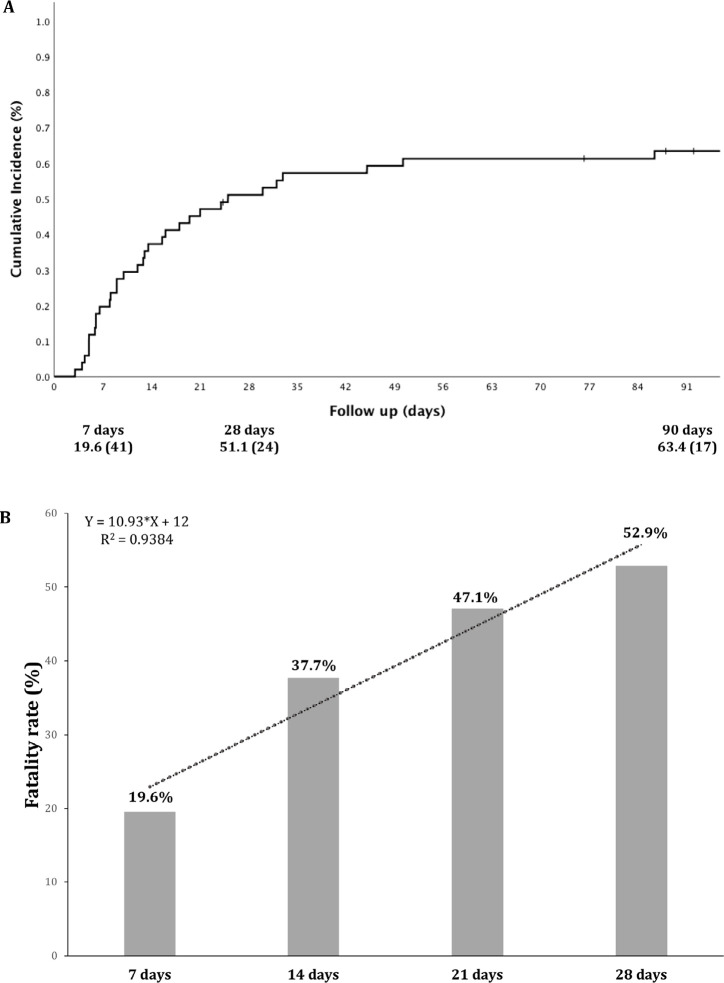
Results: The 90-day cumulative incidence of death was 63.4%. Only APACHE IV score differed between survivors and nonsurvivors: 91.2±18.3 vs. 106.5±26.3, P = 0.03. The AUC- ROC of APACHE IV for predicting death was 0.706 (P = 0.04) and 0.656 (P = 0.06) at 7 and 90 days, respectively. Receiving a kidney from a deceased donor (HR = 3.16; P = 0.03), troponin levels at admission (HR for each ng/mL = 1.001; P = 0.03), APACHE IV score (HR for each 1 point = 1.02; P = 0.01), mechanical ventilation (MV) requirement (HR = 3.04; P = 0.002) and vasopressor use on the first day after ICU admission (HR = 3.85; P < 0.001) were associated with the 90-day mortality in the univariate analysis.
Conclusion: KT recipients had high mortality, which was associated with type of donor, troponin levels, early use of vasopressors, and MV requirement. The other traditional severity scores investigated could not predict mortality.
Introdução:: a capacidade preditiva dos escores de gravidade para mortalidade em pacientes admitidos em unidades de terapia intensiva não é bem conhecida entre pacientes transplantados renais (TR), especialmente aqueles diagnosticados com doença coronavírus 2019 (COVID-19). Este estudo avaliou a capacidade preditiva dos escores de gravidade para mortalidade em receptores de TR.
Métodos:: Foram inscritos 51 receptores de TR diagnosticados com COVID-19. O desempenho das ferramentas SOFA, SAPS 3, APACHE IV em predizer mortalidade após COVID-19 foi comparado pela área sob a curva ROC (AUC-ROC) e realizou-se análise de regressão univariada de Cox.
Resultados:: A incidência cumulativa de óbito em 90 dias foi 63,4%. Somente APACHE IV diferiu entre sobreviventes e não-sobreviventes: 91,2±18,3 vs. 106,5±26,3; P = 0,03. A AUC-ROC do APACHE IV para predizer óbito foi 0,706 (P = 0,04) e 0,656 (P = 0,06) aos 7 e 90 dias, respectivamente. Receber rim de doador falecido (HR = 3,16; P = 0,03), níveis de troponina na admissão (HR para cada ng/mL = 1,001; P = 0,03), escore APACHE IV (HR para cada 1 ponto = 1,02; P = 0,01), necessidade de ventilação mecânica (VM) (HR = 3,04; P = 0,002), uso de vasopressor no primeiro dia após admissão na UTI (HR = 3,85; P < 0,001) foram associados à mortalidade em 90 dias na análise univariada.
Conclusão:: Receptores de TR apresentaram alta mortalidade, associada ao tipo de doador, níveis de troponina, uso precoce de vasopressores e necessidade de VM. Os outros escores tradicionais de gravidade investigados não puderam predizer mortalidade.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures

References
-
- World Health Organization (WHO) Weekly epidemiological update - 19 January 2021 [Internet] Geneva: WHO; 2021. [access in 2021 Feb 07]. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update---... .
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA. 2020 Apr;323(13):1239–42. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
