

Model-informed drug development supporting the approval of the avelumab flat-dose regimen in patients with advanced renal cell carcinoma
- PMID: 35166465
- PMCID: PMC9007597
- DOI: 10.1002/psp4.12771
Model-informed drug development supporting the approval of the avelumab flat-dose regimen in patients with advanced renal cell carcinoma
Abstract
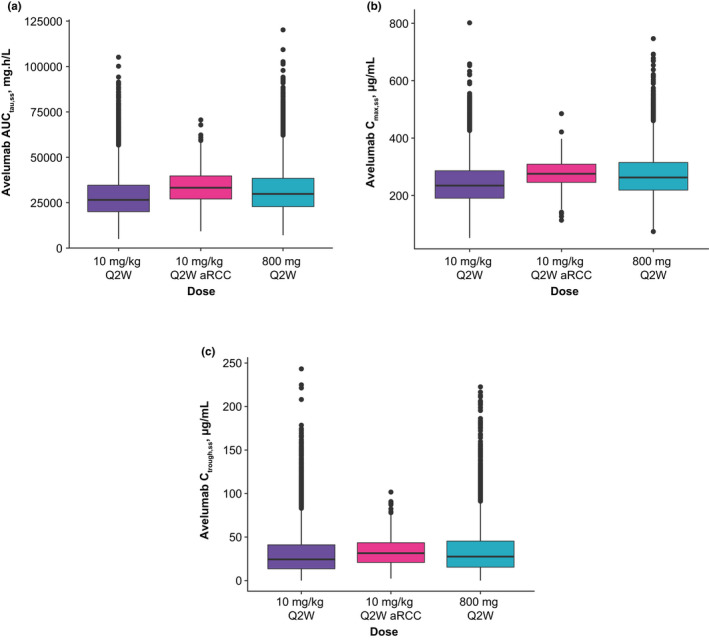
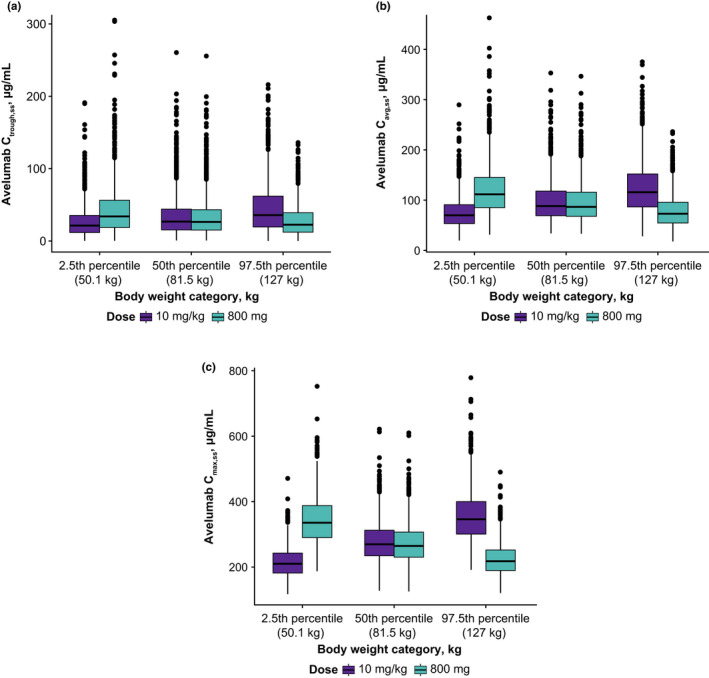
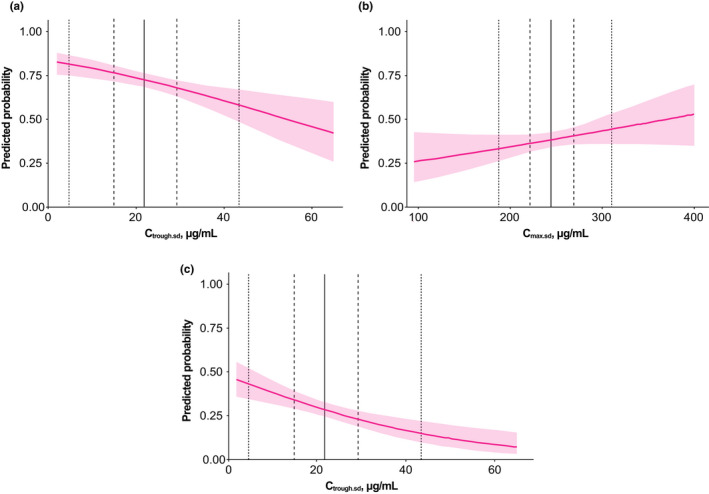
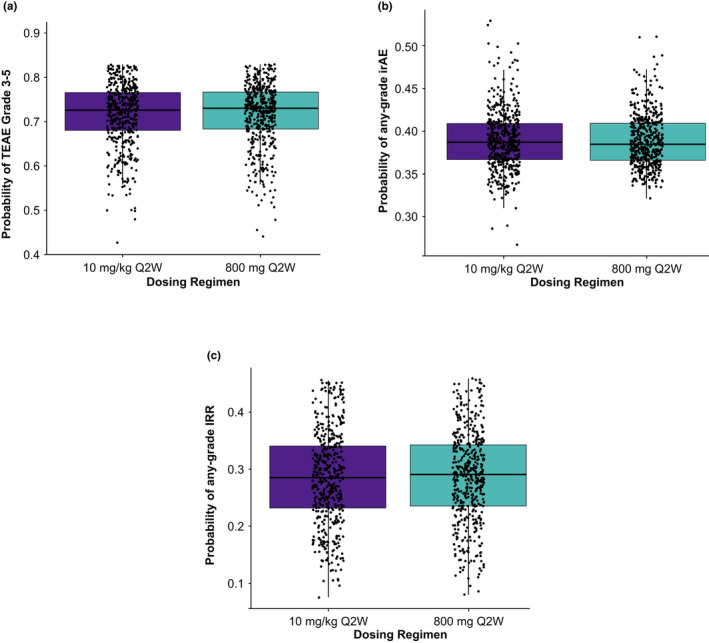
Avelumab is an anti-PD-L1 monoclonal antibody approved as monotherapy for Merkel cell carcinoma (MCC) and urothelial carcinoma (UC), and in combination with axitinib for advanced renal cell carcinoma (aRCC). Although initially approved with weight-based dosing (10 mg/kg intravenously [IV] every 2 weeks [Q2W]), avelumab was subsequently approved for flat dosing (800 mg IV Q2W) based on population pharmacokinetic (PopPK), exposure-efficacy, and exposure-safety modeling in MCC and UC. Here, through modeling and simulation, we provide justification for a flat-dose regimen of avelumab plus axitinib in aRCC. Simulated exposure metrics from the previous monotherapy PopPK model (1827 patients) for both weight-based and flat-dose regimens were compared with exposure metrics from treatment-naive patients with aRCC who received avelumab plus axitinib (488 patients). The aRCC population exposures were derived from a fit-for-purpose PopPK model developed using data from monotherapy and combination studies and the existing base structural PopPK model. Exposure-response relationships for safety were analyzed, including grade ≥3 treatment-emergent adverse events (TEAEs), any-grade infusion-related reactions, and TEAE any-grade immune-related adverse events (irAEs). Weight-based dosing of avelumab in the aRCC population yielded similar PK exposures to the flat-dose regimen reference exposures in the monotherapy population. Increased avelumab exposure was not associated with increased probabilities of grade ≥3 TEAEs or any-grade IRRs, although there was a weak association with an increased probability of any-grade irAEs. Overall, models in aRCC suggest that the avelumab 800-mg Q2W flat-dose regimen would provide similar benefits compared with weight-based dosing with no meaningful change in the probability of AEs.
Trial registration: ClinicalTrials.gov NCT02684006 NCT02493751.
© 2022 The Authors. CPT: Pharmacometrics & Systems Pharmacology published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
J.C. Masters and A. di Pietro are employees of Pfizer, and own stock and other ownership interests in Pfizer. A. Khandelwal is an employee of the healthcare business of Merck KGaA, Darmstadt, Germany, owns stock and other ownership interests in Merck KGaA, Darmstadt, Germany, and holds patents, royalties, or other intellectual property in the healthcare business of Merck KGaA, Darmstadt, Germany. H. Dai is an employee of EMD Serono, and owns stock and other ownership interests in Merck KGaA, Darmstadt, Germany. S. Brar was an employee of Pfizer.
Figures
References
-
- Hamilton G, Rath B. Avelumab: combining immune checkpoint inhibition and antibody‐dependent cytotoxicity. Expert Opin Biol Ther. 2017;17:515‐523. - PubMed
-
- Bavencio (avelumab) . Prescribing Information. EMD Serono; 2020.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
