

Myocardial Injury Pattern at MRI in COVID-19 Vaccine-Associated Myocarditis
- PMID: 35166587
- PMCID: PMC8856022
- DOI: 10.1148/radiol.212559
Myocardial Injury Pattern at MRI in COVID-19 Vaccine-Associated Myocarditis
Abstract
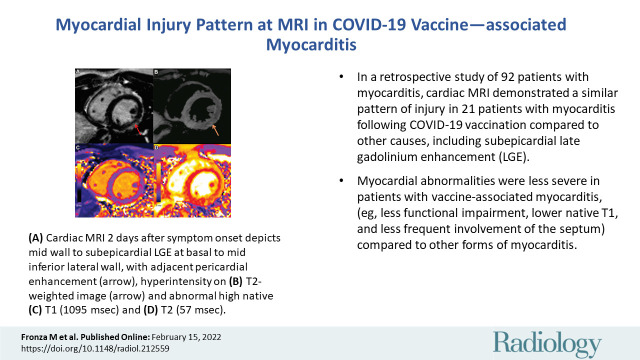
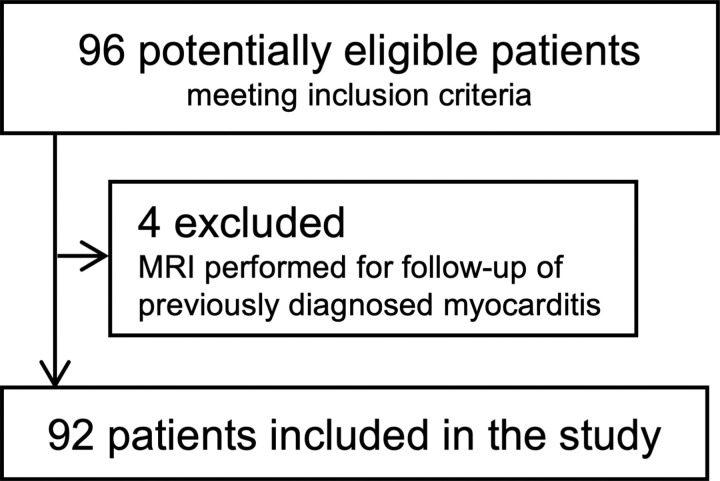
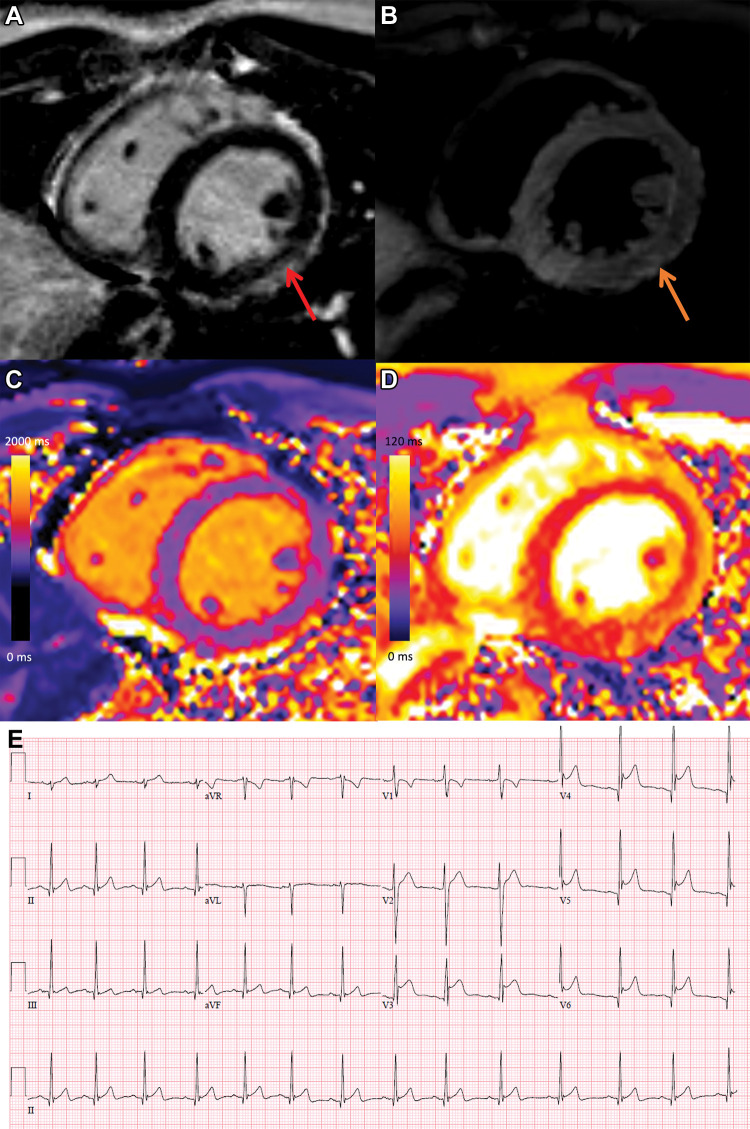
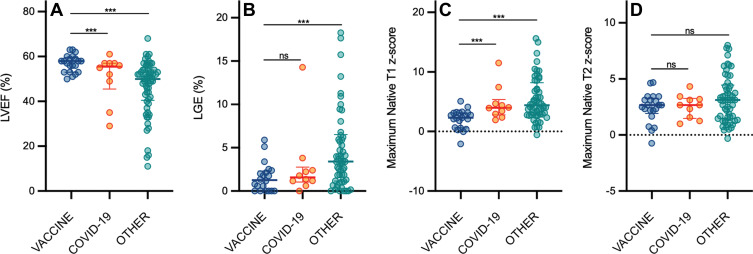
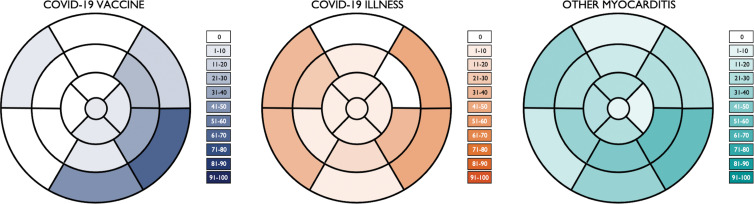
Background There are limited data on the pattern and severity of myocardial injury in patients with COVID-19 vaccination-associated myocarditis. Purpose To describe myocardial injury following COVID-19 vaccination and to compare these findings to other causes of myocarditis. Materials and Methods In this retrospective cohort study, consecutive adult patients with myocarditis with at least one T1-based and at least one T2-based abnormality at cardiac MRI performed at a tertiary referral hospital from December 2019 to November 2021 were included. Patients were classified into one of three groups: myocarditis following COVID-19 vaccination, myocarditis following COVID-19 illness, and other myocarditis not associated with COVID-19 vaccination or illness. Results Of the 92 included patients, 21 (23%) had myocarditis following COVID-19 vaccination (mean age, 31 years ± 14 [SD]; 17 men; messenger RNA-1273 in 12 [57%] and BNT162b2 in nine [43%]). Ten of 92 (11%) patients had myocarditis following COVID-19 illness (mean age, 51 years ± 14; three men) and 61 of 92 (66%) patients had other myocarditis (mean age, 44 years ± 18; 36 men). MRI findings in the 21 patients with vaccine-associated myocarditis included late gadolinium enhancement (LGE) in 17 patients (81%) and left ventricular dysfunction in six (29%). Compared with other causes of myocarditis, patients with vaccine-associated myocarditis had a higher left ventricular ejection fraction and less extensive LGE, even after controlling for age, sex, and time from symptom onset to MRI. The most frequent location of LGE in all groups was subepicardial at the basal inferolateral wall, although septal involvement was less common in vaccine-associated myocarditis. At short-term follow-up (median, 22 days [IQR, 7-48 days]), all patients with vaccine-associated myocarditis were asymptomatic with no adverse events. Conclusion Cardiac MRI demonstrated a similar pattern of myocardial injury in vaccine-associated myocarditis compared with other causes, although abnormalities were less severe, with less frequent septal involvement and no adverse events over the short-term follow-up. © RSNA, 2022 Online supplemental material is available for this article. See also the editorial by Raman and Neubauer in this issue.
Conflict of interest statement
Figures
Comment in
-
Postvaccine Myocarditis: A Risk Worth the Reward?Radiology. 2022 Sep;304(3):563-565. doi: 10.1148/radiol.220252. Epub 2022 Feb 15. Radiology. 2022. PMID: 35166589 Free PMC article. No abstract available.
References
-
- Aretz HT , Billingham ME , Edwards WD , et al . Myocarditis. A histopathologic definition and classification . Am J Cardiovasc Pathol 1987. ; 1 ( 1 ): 3 – 14 . - PubMed
-
- Ammirati E , Cipriani M , Moro C , et al . Clinical Presentation and Outcome in a Contemporary Cohort of Patients With Acute Myocarditis: Multicenter Lombardy Registry . Circulation 2018. ; 138 ( 11 ): 1088 – 1099 . - PubMed
-
- Su JR , McNeil MM , Welsh KJ , et al . Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990-2018 . Vaccine 2021. ; 39 ( 5 ): 839 – 845 . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
