

Effect of Offering Care Management or Online Dialectical Behavior Therapy Skills Training vs Usual Care on Self-harm Among Adult Outpatients With Suicidal Ideation: A Randomized Clinical Trial
- PMID: 35166800
- PMCID: PMC8848197
- DOI: 10.1001/jama.2022.0423
Effect of Offering Care Management or Online Dialectical Behavior Therapy Skills Training vs Usual Care on Self-harm Among Adult Outpatients With Suicidal Ideation: A Randomized Clinical Trial
Abstract
Importance: People at risk of self-harm or suicidal behavior can be accurately identified, but effective prevention will require effective scalable interventions.
Objective: To compare 2 low-intensity outreach programs with usual care for prevention of suicidal behavior among outpatients who report recent frequent suicidal thoughts.
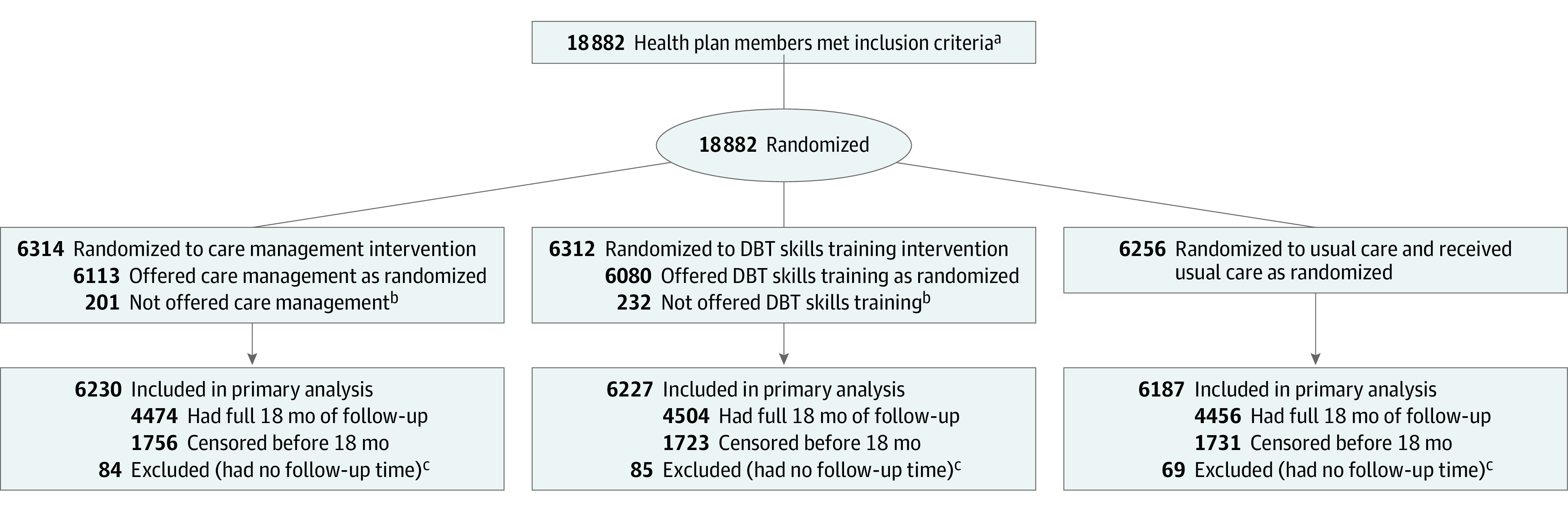
Design, setting, and participants: Pragmatic randomized clinical trial including outpatients reporting frequent suicidal thoughts identified using routine Patient Health Questionnaire depression screening at 4 US integrated health systems. A total of 18 882 patients were randomized between March 2015 and September 2018, and ascertainment of outcomes continued through March 2020.
Interventions: Patients were randomized to a care management intervention (n = 6230) that included systematic outreach and care, a skills training intervention (n = 6227) that introduced 4 dialectical behavior therapy skills (mindfulness, mindfulness of current emotion, opposite action, and paced breathing), or usual care (n = 6187). Interventions, lasting up to 12 months, were delivered primarily through electronic health record online messaging and were intended to supplement ongoing mental health care.
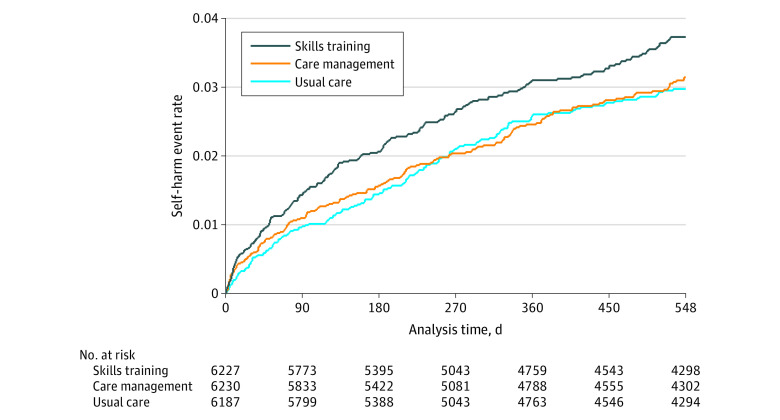
Main outcomes and measures: The primary outcome was time to first nonfatal or fatal self-harm. Nonfatal self-harm was ascertained from health system records, and fatal self-harm was ascertained from state mortality data. Secondary outcomes included more severe self-harm (leading to death or hospitalization) and a broader definition of self-harm (selected injuries and poisonings not originally coded as self-harm).
Results: A total of 18 644 patients (9009 [48%] aged 45 years or older; 12 543 [67%] female; 9222 [50%] from mental health specialty clinics and the remainder from primary care) contributed at least 1 day of follow-up data and were included in analyses. Thirty-one percent of participants offered care management and 39% offered skills training actively engaged in intervention programs. A total of 540 participants had a self-harm event (including 45 deaths attributed to self-harm and 495 nonfatal self-harm events) over 18 months following randomization: 172 (3.27%) in care management, 206 (3.92%) in skills training, and 162 (3.27%) in usual care. Risk of fatal or nonfatal self-harm over 18 months did not differ significantly between the care management and usual care groups (hazard ratio [HR], 1.07; 97.5% CI, 0.84-1.37) but was significantly higher in the skills training group than in usual care (HR, 1.29; 97.5% CI, 1.02-1.64). For severe self-harm, care management vs usual care had an HR of 1.03 (97.5% CI, 0.71-1.51); skills training vs usual care had an HR of 1.34 (97.5% CI, 0.94-1.91). For the broader self-harm definition, care management vs usual care had an HR of 1.10 (97.5% CI, 0.92-1.33); skills training vs usual care had an HR of 1.17 (97.5% CI, 0.97-1.41).
Conclusions and relevance: Among adult outpatients with frequent suicidal ideation, offering care management did not significantly reduce risk of self-harm, and offering brief dialectical behavior therapy skills training significantly increased risk of self-harm, compared with usual care. These findings do not support implementation of the programs tested in this study.
Trial registration: ClinicalTrials.gov Identifier: NCT02326883.
Conflict of interest statement
Figures
Comment in
-
Health System-Based Low-Intensity Interventions to Prevent Self-harm Among Patients With Suicidal Ideation: Disentangling the Effects of Implementation Strategies and Interventions.JAMA. 2022 Feb 15;327(7):626-628. doi: 10.1001/jama.2022.0770. JAMA. 2022. PMID: 35166818 No abstract available.
-
Effect of Care Management or Online Dialectical Behavior Therapy Skills Training vs Usual Care on Self-harm Among Adults With Suicidal Ideation.JAMA. 2022 Jun 14;327(22):2246. doi: 10.1001/jama.2022.5880. JAMA. 2022. PMID: 35699711 No abstract available.
-
Effect of Care Management or Online Dialectical Behavior Therapy Skills Training vs Usual Care on Self-harm Among Adults With Suicidal Ideation.JAMA. 2022 Jun 14;327(22):2245-2246. doi: 10.1001/jama.2022.5877. JAMA. 2022. PMID: 35699712 No abstract available.
-
Effect of Care Management or Online Dialectical Behavior Therapy Skills Training vs Usual Care on Self-harm Among Adults With Suicidal Ideation.JAMA. 2022 Jun 14;327(22):2245. doi: 10.1001/jama.2022.5874. JAMA. 2022. PMID: 35699713 No abstract available.
References
-
- The Joint Commission Patient Safety Advisory Group . Detecting and Treating Suicidal Ideation in All Settings. The Joint Commission; 2016. The Joint Commission Sentinel Event Alert 56.
