

Factors influencing the functional status of aortic valve in ovine models supported by continuous-flow left ventricular assist device
- PMID: 35167127
- PMCID: PMC9310577
- DOI: 10.1111/aor.14207
Factors influencing the functional status of aortic valve in ovine models supported by continuous-flow left ventricular assist device
Abstract
Objectives: An acute animal experiment was performed to observe factors influencing the functional status of the aortic valve functional status after continuous-flow left ventricular assist device (CF-LVAD) implantation in an ovine model, and a physiologic predictive model was established.
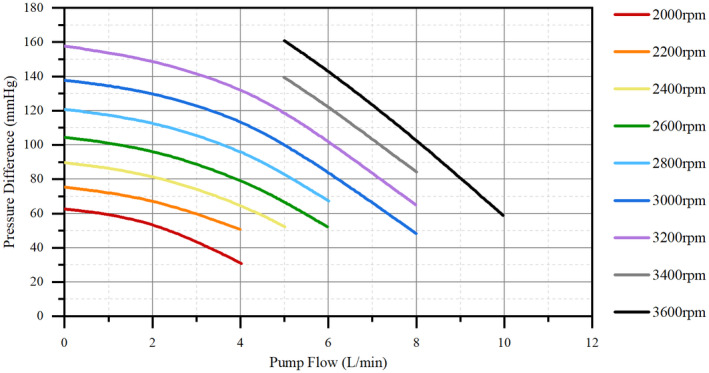
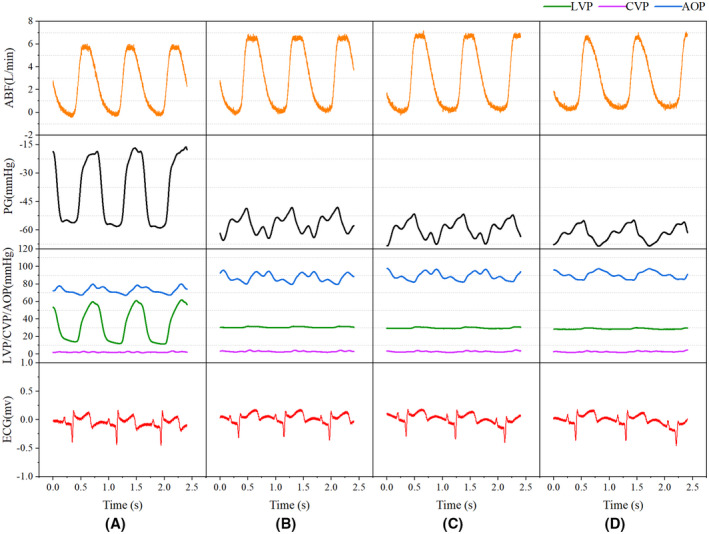
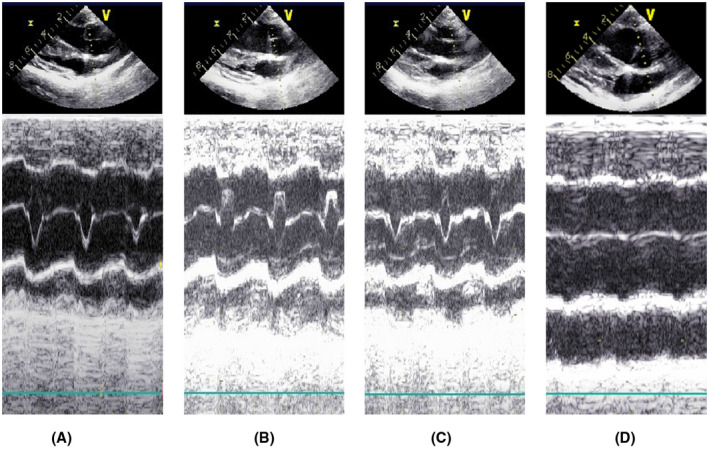
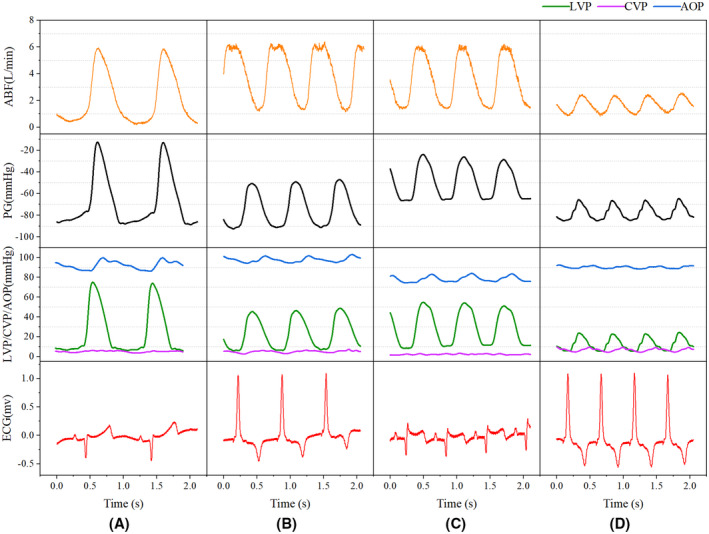
Methods: A CF-LVAD model was established in Small Tail Han sheep. The initial heart rate (HR) was set to 60 beats/min, and grouping was performed at an interval of 20 beats/min. In all groups, the pump speed was started from 2000 rpm and was gradually increased by 50-100 rpm. A multi-channel physiological recorder recorded the HR, aortic pressure, central venous pressure, and left ventricular systolic pressure (LVSP). A double-channel ultrasonic flowmeter was used to obtain real-time artificial vascular blood flow (ABF). A color Doppler ultrasound device was applied to assess the aortic valve functional status. Multivariate dichotomous logistic regression was used to screen significant variables for predicting the functional status of the aortic valve.
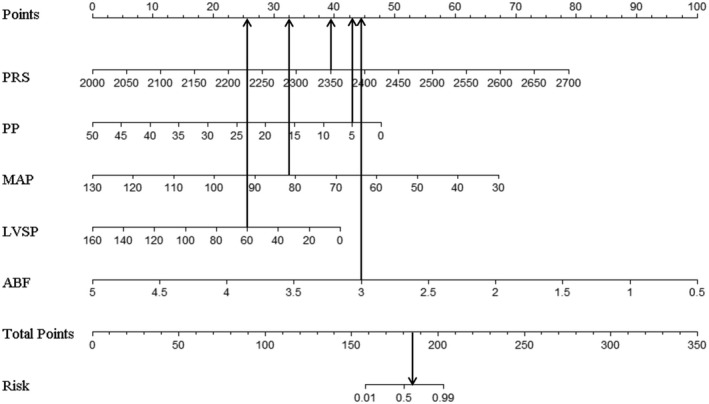
Results: Observational studies showed that ABF and the risk of aortic valve closure (AVC) were positively correlated with pump speed at the same HR. Meanwhile, the mean arterial pressure (MAP) was unaltered or slightly increased with increased pump speed. When the pump speed was constant, an increase in HR was associated with a decrease in the size of the aortic valve opening. This phenomenon was accompanied by an initial transient increase in the ABF and MAP, which subsequently decreased. Statistical analysis showed that the AVC was associated with increased pump speed (OR = 1.02, 95% CI = 1.01-1.04, p = 0.001), decreased LVSP (OR = 0.95, 95% CI = 0.91-0.98, p = 0.003), and decreased pulse pressure (OR = 0.82, 95% CI = 0.68-0.96, p = 0.026). ABF or MAP was negatively associated with the risk of AVC (OR < 1). The prediction model of AVC after CF-LVAD implantation exhibited good differentiation (AUC = 0.973, 95% CI = 0.978-0.995) and calibration performance (Hosmer-Lemeshow χ2 = 9.834, p = 0.277 > 0.05).
Conclusions: The pump speed, LVSP, ABF, MAP, and pulse pressure are significant predictors of the risk of AVC. Predictive models built from these predictors yielded good performance in differentiating aortic valve opening and closure after CF-LVAD implantation.
Keywords: LVAD; aortic valve; influencing factors; nomogram; predictive model.
© 2022 The Authors. Artificial Organs published by International Center for Artificial Organ and Transplantation (ICAOT) and Wiley Periodicals LLC.
Conflict of interest statement
All authors had no conflicts of interest to disclose.
Figures





References
-
- Molina EJ, Shah P, Kiernan MS, Cornwell WK 3rd, Copeland H, Takeda K, et al. The society of thoracic surgeons Intermacs 2020 annual report. Ann Thorac Surg. 2021;111(3):778–92. - PubMed
-
- Teuteberg JJ, Cleveland JC Jr, Cowger J, Higgins RS, Goldstein DJ, Keebler M, et al. The society of thoracic surgeons Intermacs 2019 annual report: the changing landscape of devices and indications. Ann Thorac Surg. 2020;109(3):649–60. - PubMed
-
- John R, Mantz K, Eckman P, Rose A, May‐Newman K. Aortic valve pathophysiology during left ventricular assist device support. J Heart Lung Transplant. 2010;29(12):1321–9. - PubMed
-
- Tuzun E, Pennings K, van Tuijl S, de Hart J, Stijnen M, van de Vosse F, et al. Assessment of aortic valve pressure overload and leaflet functions in an ex vivo beating heart loaded with a continuous flow cardiac assist device. Eur J Cardiothorac Surg. 2014;45(2):377–83. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
