

Different types of emollient cream exhibit diverse physiological effects on the skin barrier in adults with atopic dermatitis
- PMID: 35167133
- PMCID: PMC9322554
- DOI: 10.1111/ced.15141
Different types of emollient cream exhibit diverse physiological effects on the skin barrier in adults with atopic dermatitis
Abstract
Background: Eczema (atopic dermatitis; AD) is a very common itchy skin condition affecting 1 in 5 children and up to 1 in 10 adults worldwide. The skin of eczema sufferers is prone to redness, irritation and dryness because it does not form an effective barrier, i.e. the ability of the skin to stop irritants, allergens and microorganisms getting into the body. Skin barrier dysfunction is a hallmark of AD. The regular and liberal (600 g/week for an adult) use of emollients is recommended for all patients with eczema), even between episodes of itching and redness, to soften and soothe the skin. In England alone, almost 9 million prescriptions for emollient creams were issued in 2018, at a cost of over £50 million. Despite this widespread use, relatively little is known about how commonly prescribed emollient creams affect the skin's barrier, and thus the role of moisturizers in AD development and progression remains unclear. We set out to compare three different types of emollient cream and a no-treatment control.
Aim: To compare the barrier-strengthening properties of a new moisturizer containing urea and glycerol (urea-glycerol cream; UGC), with those of a glycerol-containing moisturizer (glycerol cream; GC), a simple paraffin cream (PC) with no humectant, and a no-treatment control (NTC).
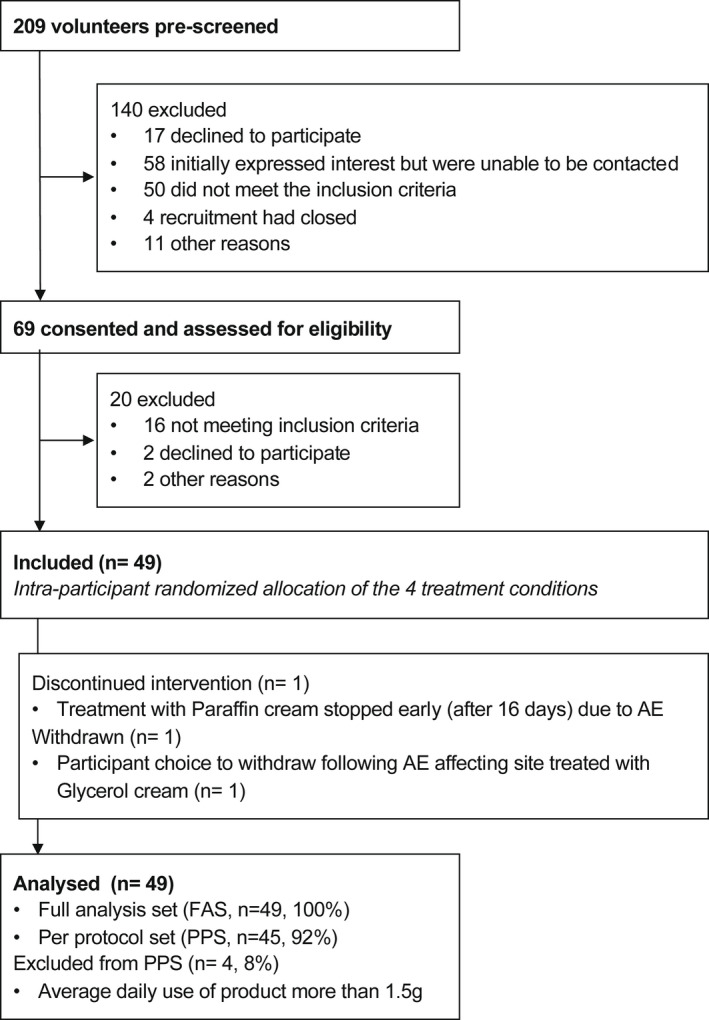
Methods: This was an observer-blinded prospective Phase 2 within-subject multilateral single-centre randomized controlled trial in adults with AD (Clinical Trials #NCT03901144). The intervention involved 4 weeks of treatment, twice daily, with the three products applied to one of four areas on the forearms the (the fourth area was the untreated control, randomized allocation). Skin properties [dryness, transepidermal water loss (TEWL), hydration and natural moisturizing factor (NMF) levels] were assessed before, during and after treatment to see what happened to the skin's barrier. The primary outcome was skin sensitivity to the irritant sodium lauryl sulfate (SLS) after treatment. We performed tests on the skin before and after treatment to see what happened to the skin's barrier.
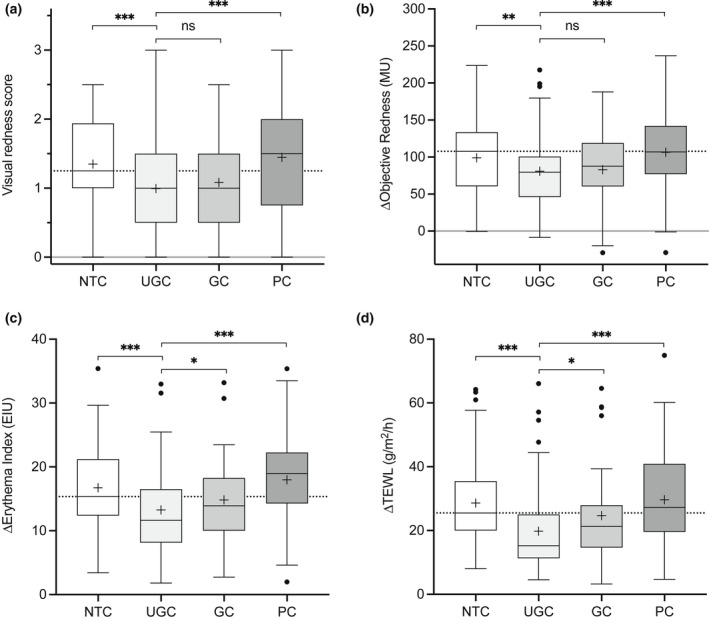
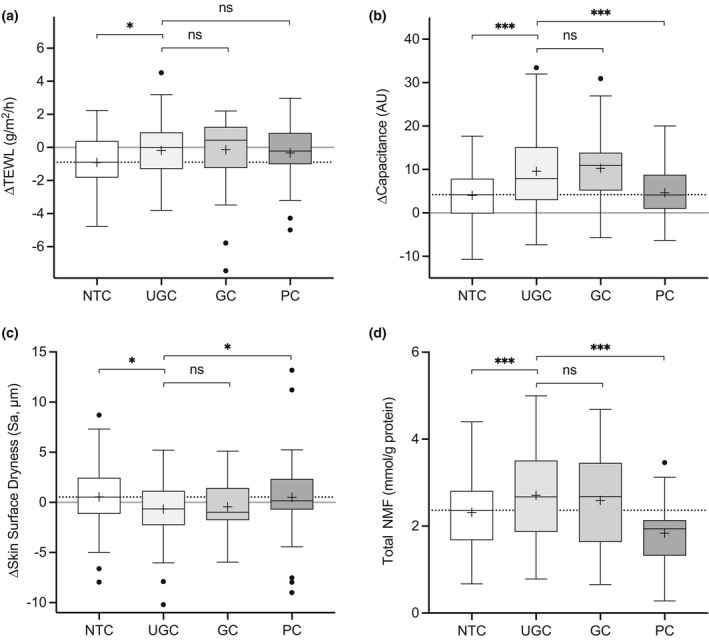
Results: In total, 49 patients were randomized, completed treatment and included in the analysis. UGC significantly reduced the response to SLS as indicated by a reduction in TEWL compared with NTC (-9.0 g/m2 /h; 95% CI -12.56 to -5.49), with PC (-9.0 g/m2 /h; 95% CI -12.60 to -5.44) and with GC -4.2 g/m2 /h; 95% CI 7.76 to -0.63). Skin moisturization improved at sites treated with UGC compared with NTC and PC, and this was accompanied by concordant changes in dryness and NMF levels. Subgroup analysis suggested FLG-dependent enhancement of treatment effects.
Conclusion: The study showed that not all emollient creams for eczema are equal. The simple paraffin-based emollient, which represents the most widely prescribed type of emollient cream in England, had no effect on the skin's barrier and reduced the skin's NMF. UGC markedly improved the skin's barrier and protected against irritation. GC performed better than PC, but not as well as UGC. UGC strengthened the skin barrier through a mechanism involving increased NMF levels in the skin, and imparted protection from SLS-induced irritation. By helping correct a major pathophysiological process, UGC has the potential to improve the long-term control of AD. The results show that different emollient creams have different effects on our skin, and only certain types have the ability to improve the skin's barrier and protect against irritants that trigger eczema.
© 2022 The Authors. Clinical and Experimental Dermatology published by John Wiley & Sons Ltd on behalf of British Association of Dermatologists.
Conflict of interest statement
SGD has received research grants from, participated in advisory boards for, or has consulted with Almirall, Astellas Pharma, Bayer, Harvey Water Softeners, Hyphens Pharma, Leo Pharma, L'Oreal, Johnson & Johnson, MSD, Perrigo, Pfizer and Stiefel‐GSK. MJC is an investigator and consultant for Astellas, Almirall, Bayer, Boots, Galapagos, Hyphens, Johnson & Johnson, Leo Pharma, L'Oreal, Menlo, MSD, Novartis, Oxagen, Pfizer, Procter & Gamble, Perrigo, Regeneron Pharmaceuticals, Inc., Sanofi Genzyme and Stiefel‐GSK. AF, KC and TH are in the employment of Perrigo Nordic who funded this study and manufacture UGC and GC. PVA, RNT, LJK, KB, JC and IU declare no conflicts of interest. Treatment with a skin barrier strengthening cream has been shown to prevent relapse of AD. By contrast, some emollients, such as aqueous cream, disrupt the skin barrier and induce adverse skin reactions. Early emollient interventions to prevent the development of AD have yielded conflicting findings. A comparison of the effects of key classes of emollients, to each other and to untreated skin, on the skin barrier is needed. A simple paraffin‐based cream did not provide any skin benefits compared with no treatment and reduced the amount of NMFs. A moisturizer containing urea and glycerol exhibited barrier‐strengthening effects, imparted greater skin moisturization and protected the skin from irritation. The different effects of emollients on the skin barrier contribute to our understanding of why they are associated with different clinical outcomes, raising the importance of emollient choice. Not all emollients exhibit skin barrier‐strengthening effects, highlighting their different therapeutic potential for treating and preventing conditions driven by skin barrier defects, such as AD.
Figures
References
-
- Wollenberg A, Christen‐Zäch S, Taieb A et al. ETFAD/EADV Eczema Task Force 2020 position paper on diagnosis and treatment of atopic dermatitis in adults and children. J Eur Acad Dermatol Venereol 2020; 34: 2717–44. - PubMed
-
- Kelleher MM, Cro S, Van Vogt E et al. Skincare interventions in infants for preventing eczema and food allergy: a cochrane systematic review and individual participant data meta‐analysis. Clin Exp Allergy 2021; 51: 402–18. - PubMed
-
- Loden M, Andersson AC, Andersson C et al. Instrumental and dermatologist evaluation of the effect of glycerine and urea on dry skin in atopic dermatitis. Skin Res Technol 2001; 7: 209–13. - PubMed
-
- Danby SG, Chalmers J, Brown K et al. A functional mechanistic study of the effect of emollients on the structure and function of the skin barrier. Br J Dermatol 2016; 175 : 1011–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
