

Knowledge, Attitudes, and Practices in the Orthopaedic Care of Sexual and Gender Minority Youth: A Survey of Two Pediatric Academic Hospitals
- PMID: 35167510
- PMCID: PMC9191605
- DOI: 10.1097/CORR.0000000000002143
Knowledge, Attitudes, and Practices in the Orthopaedic Care of Sexual and Gender Minority Youth: A Survey of Two Pediatric Academic Hospitals
Abstract
Background: Lesbian, gay, bisexual, transgender, and queer (LGBTQ) children and adolescents continue to experience unmet healthcare needs, partly because of clinician biases, discrimination, and inadequate education. Although clinician attitudes and knowledge related to sexual and gender minority health have been well studied in other medical specialties, these have been scarcely studied in orthopaedics.
Questions/purposes: (1) What are pediatric orthopaedic healthcare professionals' attitudes (perceived importance, openness, comfort, and confidence) toward caring for sexual and gender minority youth? (2) What do pediatric orthopaedic healthcare professionals know about caring for this patient population? (3) What factors are associated with clinician attitude and/or knowledge? (4) What existing initiatives to improve orthopaedic care for this population are clinicians aware of at their home institutions?
Methods: All 123 orthopaedic healthcare professionals at two pediatric academic hospitals in the Midwestern and Northeastern United States were sent a 34-question, internet-based, anonymous survey. The survey queried respondent demographics, attitudes, knowledge, and practice behaviors at their home institutions related to the care of sexual and gender minority youth. Respondent attitudes were queried using the Attitudes Summary Measure, which is a survey instrument that was previously validated to assess clinicians' attitudes regarding sexual and gender minority patients. Items used to assess knowledge and practice behaviors were developed by content experts in LGBTQ health and/or survey design, as well as orthopaedic surgeons to improve face validity and to mitigate push-polling. Attitude and knowledge items used a 5-point Likert scale. Sixty-six percent (81 of 123) of clinicians completed the survey. Of those, 47% (38 of 81) were physicians, 73% (59 of 81) were licensed for fewer than 20 years, 63% (51 of 81) were women, and 53% (43 of 81) described themselves as liberal-leaning. The response proportions were 73% (38 of 52) among eligible physicians specifically and 61% (43 of 71) among other clinicians (nurse practitioners, physician assistants, and registered nurses). To assess potential nonresponse bias, we compared early responders (within 2 weeks) with late responders (after 2 weeks) and found no differences in responder demographics or in questionnaire responses (all p > 0.05). The main outcome measures included responses to the attitude and knowledge questionnaire, as well as the existing practices questionnaire. To answer our research questions regarding clinician attitudes knowledge and awareness of institutional initiatives, we compared participant responses using chi-square tests, the Student t-test, and the McNemar tests, as appropriate. To answer our research question on factors associated with questionnaire responses, we reported data for each question, stratified by hospital, years since licensure, and political leaning. Comparisons were conducted across strata using chi-square tests for Likert response items and ANOVA for continuous response items. All p values less than 0.05 were considered significant.
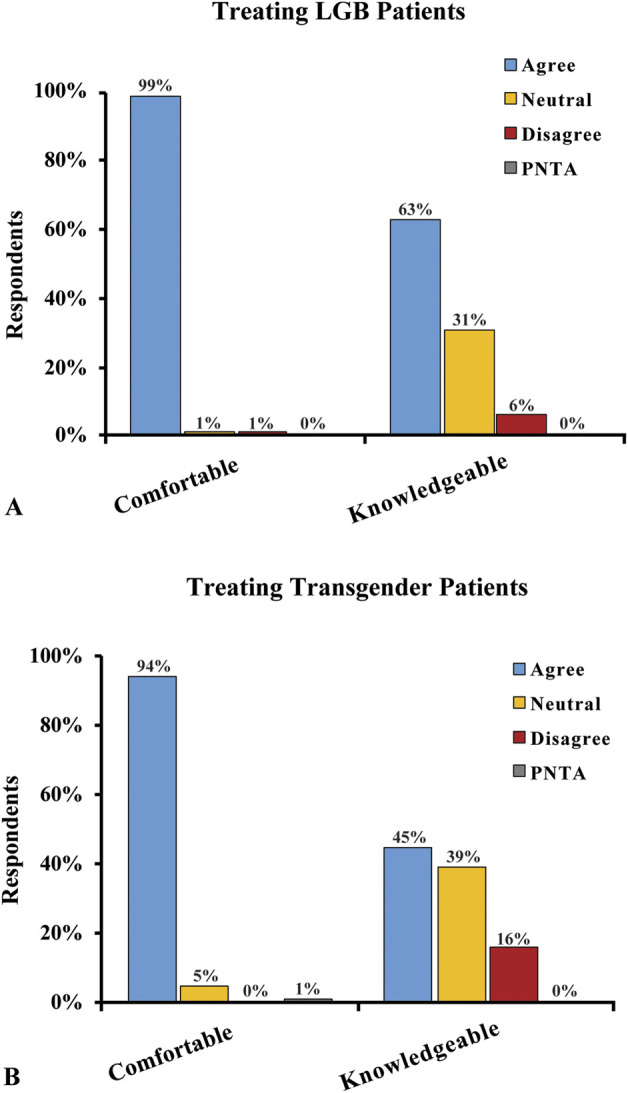
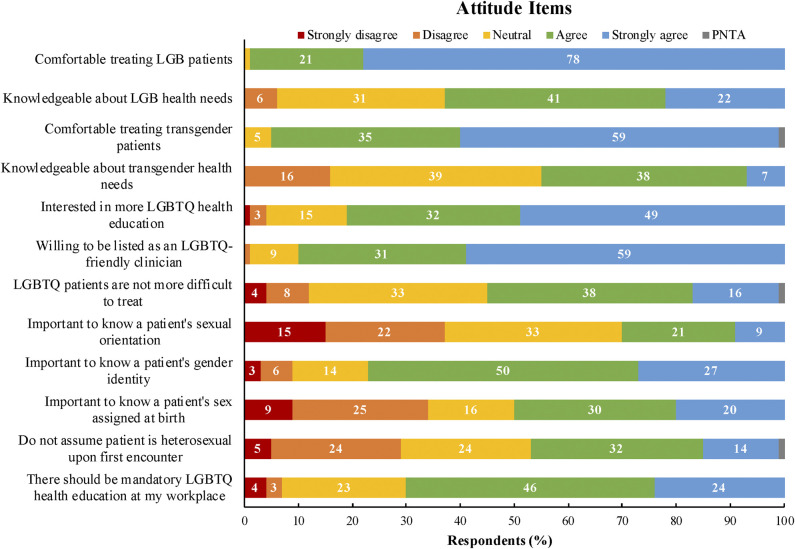
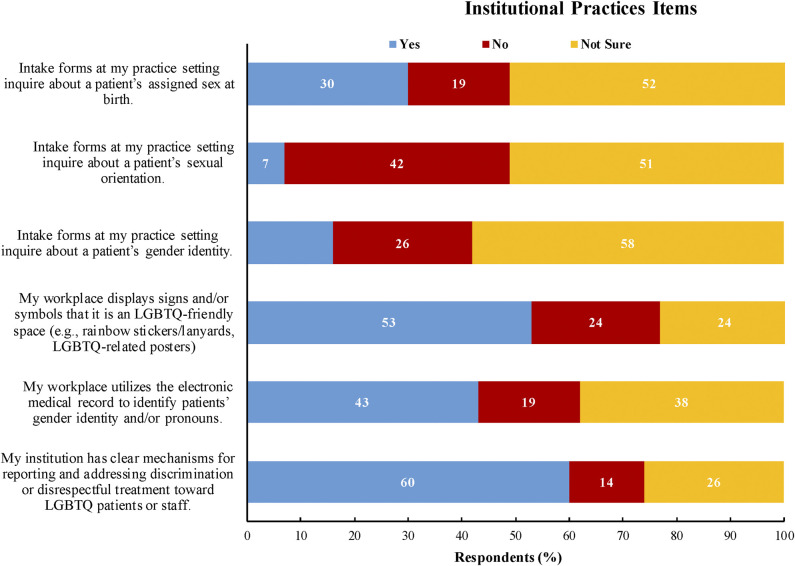
Results: Of the respondents who reported feeling comfortable treating lesbian, gay, and bisexual (sexual minority) youth, a small proportion reported feeling confident in their knowledge about these patients' health needs (99% [80 of 81] versus 63% [51 of 80], 36% reduction [95% confidence interval 23% to 47%]; p < 0.001). Similarly, of those who reported feeling comfortable treating transgender (gender minority) youth, a smaller proportion reported feeling confident in their knowledge of their health needs (94% [76 of 81] versus 49% [37 of 76], 45% reduction [95% CI 31% to 59%]; p < 0.001). There was substantial interest in receiving more education regarding the health concerns of LGBTQ people (81% [66 of 81]) and being listed as an LGBTQ-friendly clinician (90% [73 of 81]). Factors that were associated with select attitude and knowledge items were duration of licensure and political leaning; gender identity, institutional affiliation, educational degree, or having LGBTQ friends and family were not associated. Many respondents were aware of the use of clinic intake forms and the electronic medical record to collect and provide patient gender identity and sexual orientation data at their practice, as well as signage and symbols (for example, rainbow posters) to cultivate LGBTQ-welcoming clinic spaces.
Conclusion: There were varying degrees of confidence and knowledge regarding the health needs of sexual and gender minority youth among pediatric orthopaedic healthcare professionals. There was considerable interest in more focused training and better use of medical technologies to improve care for this population.
Clinical relevance: The study findings support the further investment in clinician training opportunities by healthcare administrators and orthopaedic associations related to the care of sexual and gender minority patients, as well as in the expansion of medical documentation to record and report important patient information such as pronouns and gender identity. Simultaneously, based on these findings, clinicians should engage with the increasing number of educational opportunities, explore their personal biases, and implement changes into their own practices, with the ultimate goal of providing equitable and informed orthopaedic care.
Copyright © 2022 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
References
-
- American Medical Association. Health care needs of lesbian, gay, bisexual, transgender and queer populations H-160.991. Available at: https://policysearch.ama-assn.org/policyfinder/detail/Health%20Care%20Ne.... Accessed February 24, 2021.
-
- Araoye I, He JK, Gilchrist S, Stubbs T, McGwin G, Jr, Ponce BA. A national survey of orthopaedic residents identifies deficiencies in the understanding of medical statistics. J Bone Joint Surg Am. 2020;102:e19. - PubMed
-
- Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Series B Stat Methodol. 1995;57:289-300.
MeSH terms
LinkOut - more resources
Full Text Sources
