

Racial Disparities in Adherence to Annual Lung Cancer Screening and Recommended Follow-Up Care: A Multicenter Cohort Study
- PMID: 35167781
- PMCID: PMC9447384
- DOI: 10.1513/AnnalsATS.202111-1253OC
Racial Disparities in Adherence to Annual Lung Cancer Screening and Recommended Follow-Up Care: A Multicenter Cohort Study
Abstract
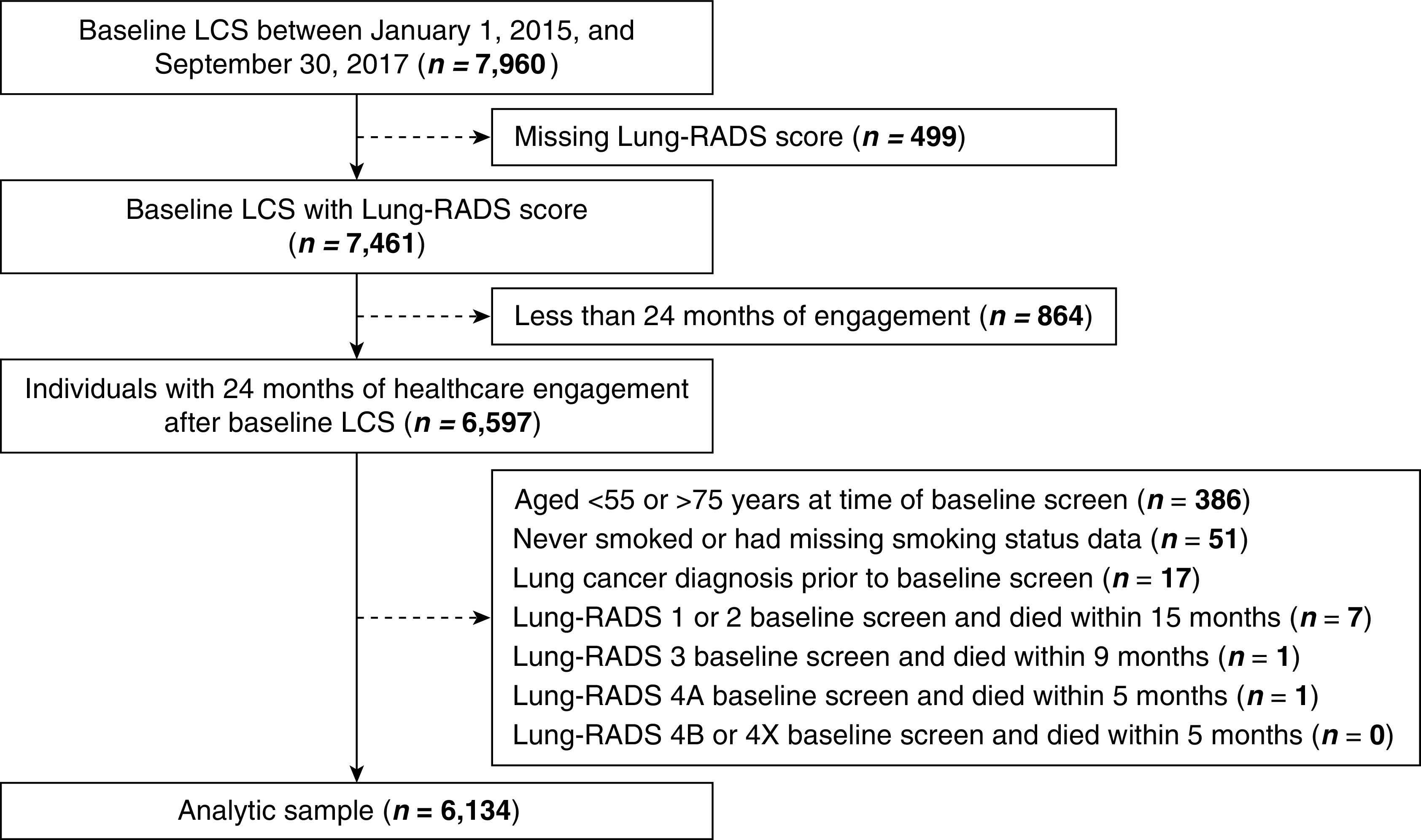
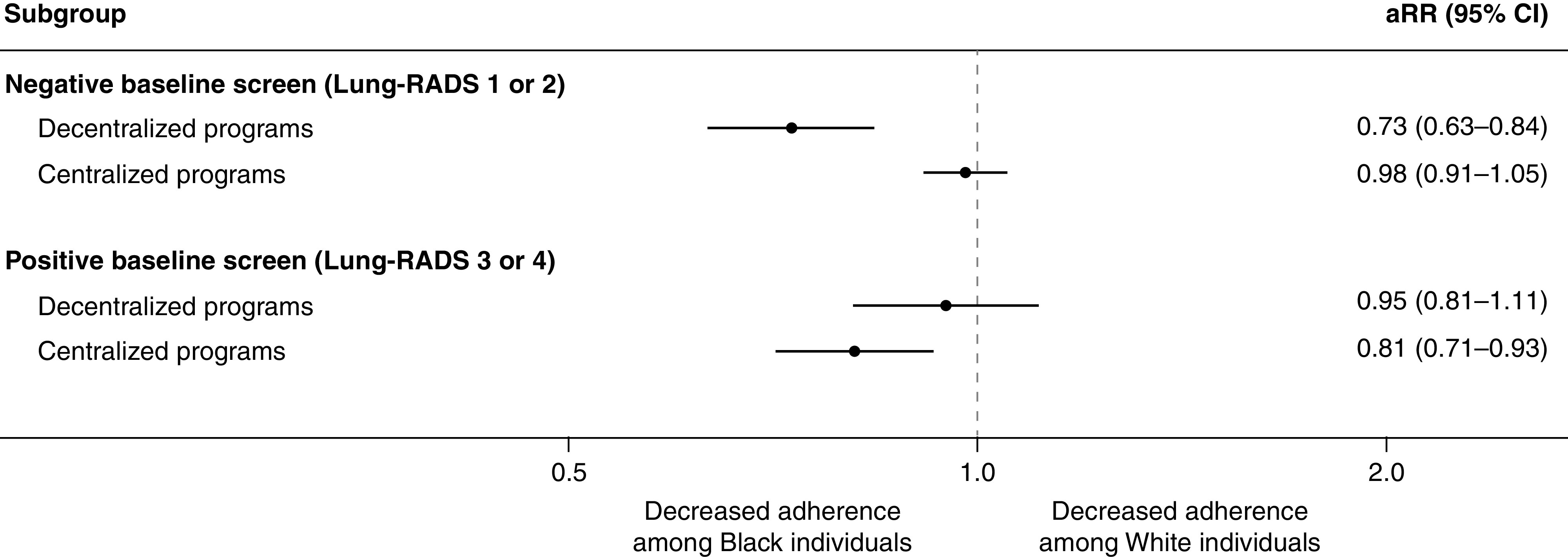
Rationale: Black patients receive recommended lung cancer screening (LCS) follow-up care less frequently than White patients, but it is unknown if this racial disparity persists across both decentralized and centralized LCS programs. Objectives: To determine adherence to American College of Radiology Lung Imaging Reporting and Data System (Lung-RADS) recommendations among individuals undergoing LCS at either decentralized or centralized programs and to evaluate the association of race with LCS adherence. Methods: We performed a multicenter retrospective cohort study of patients receiving LCS at five heterogeneous U.S. healthcare systems. We calculated adherence to annual LCS among patients with a negative baseline screen (Lung-RADS 1 or 2) and recommended follow-up care among those with a positive baseline screen (Lung-RADS 3, 4A, 4B, or 4X) stratified by type of LCS program and evaluated the association between race and adherence using multivariable modified Poisson regression. Results: Of the 6,134 total individuals receiving LCS, 5,142 (83.8%) had negative baseline screens, and 992 (16.2%) had positive baseline screens. Adherence to both annual LCS (34.8% vs. 76.1%; P < 0.001) and recommended follow-up care (63.9% vs. 74.6%; P < 0.001) was lower at decentralized compared with centralized programs. Among individuals with negative baseline screens, a racial disparity in adherence was observed only at decentralized screening programs (interaction term, P < 0.001). At decentralized programs, Black race was associated with 27% reduced adherence to annual LCS (adjusted relative risk [aRR], 0.73; 95% confidence interval [CI], 0.63-0.84), whereas at centralized programs, no effect by race was observed (aRR, 0.98; 95% CI, 0.91-1.05). In contrast, among those with positive baseline screens, there was no significant difference by race for adherence to recommended follow-up care by type of LCS program (decentralized aRR, 0.95; 95% CI, 0.81-1.11; centralized aRR, 0.81; 95% CI, 0.71-0.93; interaction term, P = 0.176). Conclusions: In this large multicenter study of individuals screened for lung cancer, adherence to both annual LCS and recommended follow-up care was greater at centralized screening programs. Black patients were less likely to receive annual LCS than White patients at decentralized compared with centralized LCS programs. Our results highlight the need for further study of healthcare system-level mechanisms to optimize longitudinal LCS care.
Keywords: early detection of cancer; guideline adherence; healthcare disparities.
Figures
Comment in
-
Addressing Lung Cancer Screening Disparities: What Does It Mean to Be Centralized?Ann Am Thorac Soc. 2022 Sep;19(9):1457-1458. doi: 10.1513/AnnalsATS.202206-495ED. Ann Am Thorac Soc. 2022. PMID: 36048121 Free PMC article. No abstract available.
References
-
- de Koning HJ, van der Aalst CM, de Jong PA, Scholten ET, Nackaerts K, Heuvelmans MA, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med . 2020;382:503–513. - PubMed
-
- Moyer VA, U.S. Preventive Services Task Force Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med . 2014;160:330–338. - PubMed
-
- American College of Radiology Committee on Lung-RADS 2021https://www.acr.org/-/media/ACR/Files/RADS/Lung-RADS/LungRADSAssessmentC....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
