

Proportional-assist ventilation with load-adjustable gain factors for mechanical ventilation: a cost-utility analysis
- PMID: 35168935
- PMCID: PMC9259387
- DOI: 10.9778/cmajo.20210078
Proportional-assist ventilation with load-adjustable gain factors for mechanical ventilation: a cost-utility analysis
Abstract
Background: Mechanical ventilation is an important component of patient critical care, but it adds expense to an already high-cost setting. This study evaluates the cost-utility of 2 modes of ventilation: proportional-assist ventilation with load-adjustable gain factors (PAV+ mode) versus pressure-support ventilation (PSV).
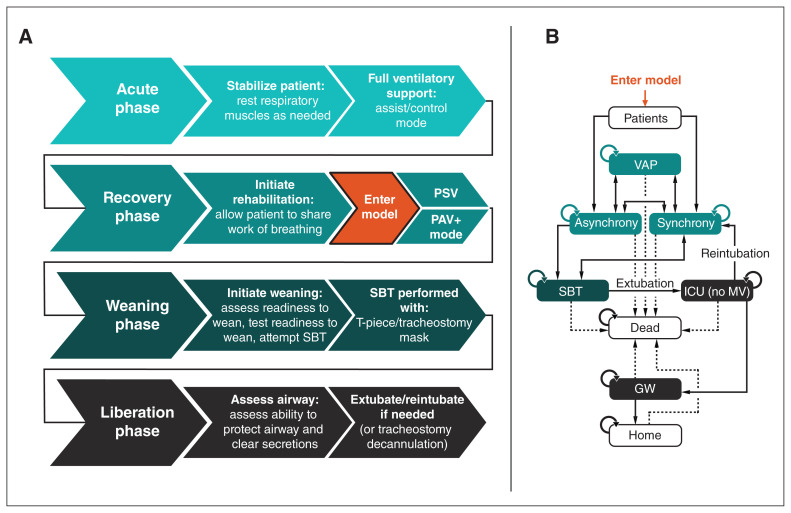
Methods: We adapted a published Markov model to the Canadian hospital-payer perspective with a 1-year time horizon. The patient population modelled includes all patients receiving invasive mechanical ventilation who have completed the acute phase of ventilatory support and have entered the recovery phase. Clinical and cost inputs were informed by a structured literature review, with the comparative effectiveness of PAV+ mode estimated via pragmatic meta-analysis. Primary outcomes of interest were costs, quality-adjusted life years (QALYs) and the (incremental) cost per QALY for patients receiving mechanical ventilation. Results were reported in 2017 Canadian dollars. We conducted probabilistic and scenario analyses to assess model uncertainty.
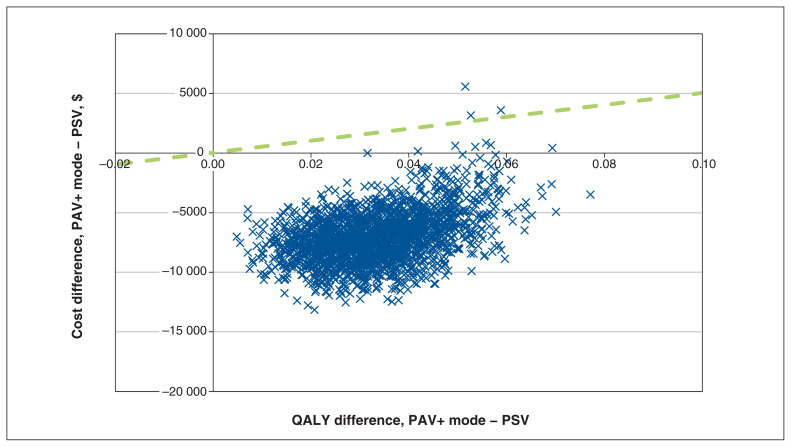
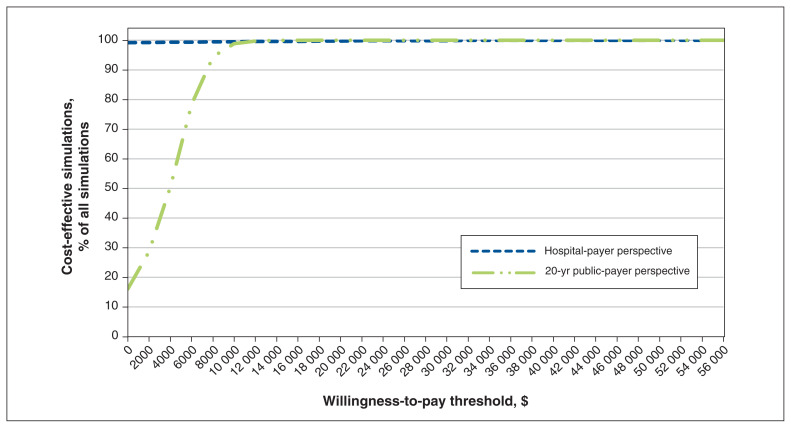
Results: Over 1 year, PSV had costs of $50 951 and accrued 0.25 QALYs. Use of PAV+ mode was associated with care costs of $43 309 and 0.29 QALYs. Compared to PSV, PAV+ mode was considered likely to be cost-effective, having lower costs (-$7642) and increased QALYs (+0.04) after 1 year. In cost-effectiveness acceptability analysis, 100% of simulations would be cost-effective at a willingness-to-pay threshold of $50 000 per QALY gained.
Interpretation: Use of PAV+ mode is expected to benefit patient care in the intensive care unit (ICU) and be a cost-effective alternative to PSV in the Canadian setting. Canadian hospital payers may therefore consider how best to optimally deliver mechanical ventilation in the ICU as they expand ICU capacity.
© 2022 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Rhodri Saunders is the owner and Jason Davis an employee of Coreva Scientific & Co, a consultancy for health economics and value-based health care. Coreva Scientific & Co received consultancy fees for its part in this research. Karen Bosma is co–principal investigator in the PROMIZING (Proportional Assist Ventilation for Minimizing the Duration of Mechanical Ventilation) clinical trial. She has previously consulted for Medtronic but received no remuneration for any part in this research project, the manuscript or any associated work. No other competing interests were declared.
Figures
References
-
- Care in Canadian ICUs. Ottawa: Canadian Institute for Health Information; 2016. [accessed 2022 Jan. 26]. Available: https://secure.cihi.ca/free_products/ICU_Report_EN.pdf.
-
- Long-term mechanical ventilation: toolkit for adult acute care providers. Toronto: Critical Care Services Ontario; 2013. [accessed 2021 Jan. 15]. Available: https://criticalcareontario.ca/wp-content/uploads/2020/10/Long-Term-Mech....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical