

Deep learning in image-based breast and cervical cancer detection: a systematic review and meta-analysis
- PMID: 35169217
- PMCID: PMC8847584
- DOI: 10.1038/s41746-022-00559-z
Deep learning in image-based breast and cervical cancer detection: a systematic review and meta-analysis
Abstract
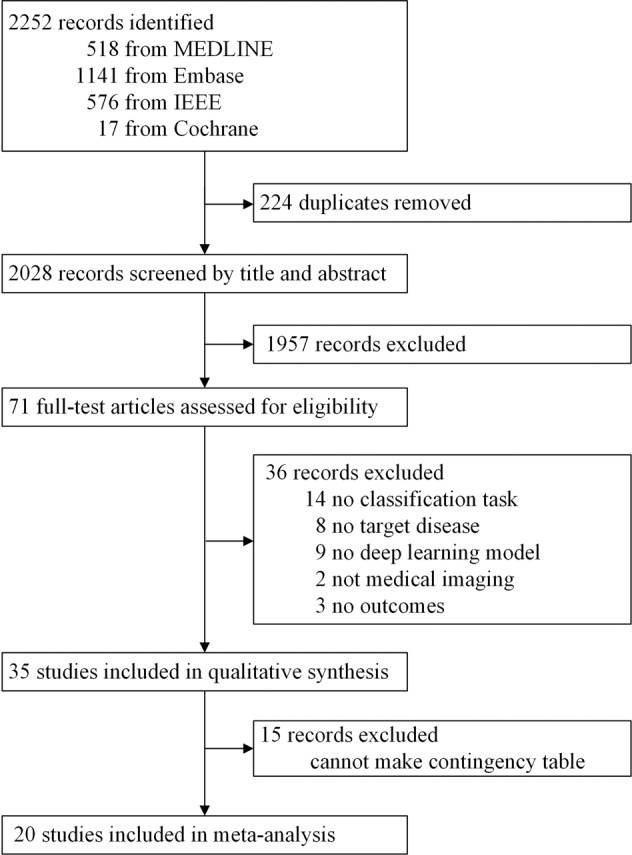
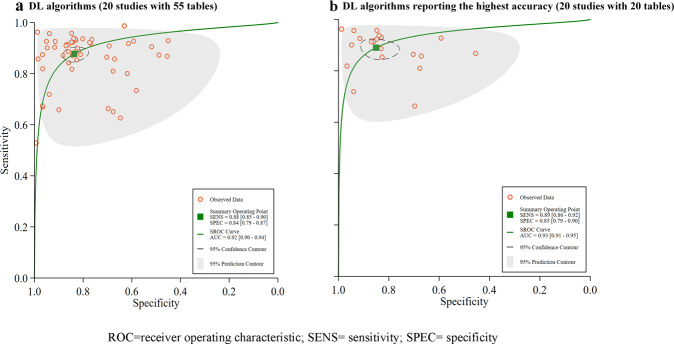
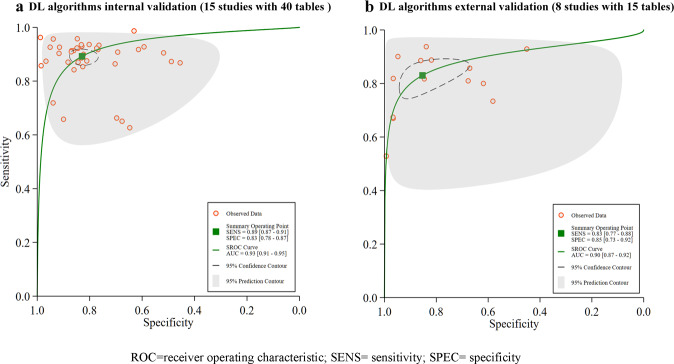
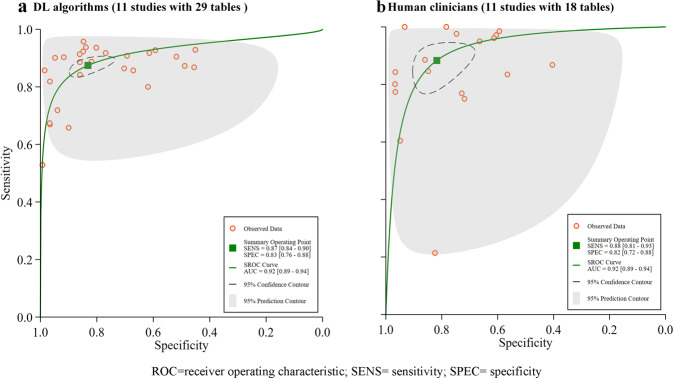
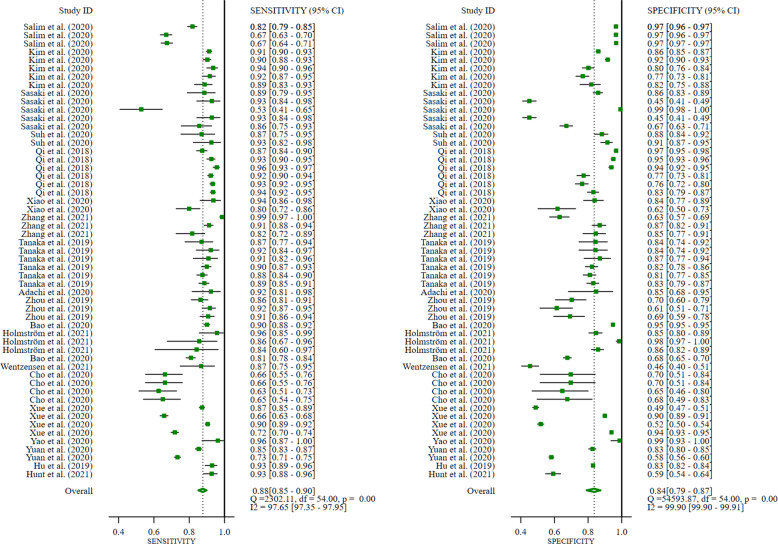
Accurate early detection of breast and cervical cancer is vital for treatment success. Here, we conduct a meta-analysis to assess the diagnostic performance of deep learning (DL) algorithms for early breast and cervical cancer identification. Four subgroups are also investigated: cancer type (breast or cervical), validation type (internal or external), imaging modalities (mammography, ultrasound, cytology, or colposcopy), and DL algorithms versus clinicians. Thirty-five studies are deemed eligible for systematic review, 20 of which are meta-analyzed, with a pooled sensitivity of 88% (95% CI 85-90%), specificity of 84% (79-87%), and AUC of 0.92 (0.90-0.94). Acceptable diagnostic performance with analogous DL algorithms was highlighted across all subgroups. Therefore, DL algorithms could be useful for detecting breast and cervical cancer using medical imaging, having equivalent performance to human clinicians. However, this tentative assertion is based on studies with relatively poor designs and reporting, which likely caused bias and overestimated algorithm performance. Evidence-based, standardized guidelines around study methods and reporting are required to improve the quality of DL research.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Sung H, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021;71:209–249. - PubMed
-
- Ginsburg O, et al. Changing global policy to deliver safe, equitable, and affordable care for women’s cancers. Lancet. 2017;389:871–880. - PubMed
LinkOut - more resources
Full Text Sources
