

Superior Long-term Appearance of Strip Craniectomy Compared with Cranial Vault Reconstruction in Metopic Craniosynostosis
- PMID: 35169528
- PMCID: PMC8830858
- DOI: 10.1097/GOX.0000000000004097
Superior Long-term Appearance of Strip Craniectomy Compared with Cranial Vault Reconstruction in Metopic Craniosynostosis
Erratum in
-
Erratum: Superior Long-term Appearance of Strip Craniectomy Compared with Cranial Vault Reconstruction in Metopic Craniosynostosis: Erratum.Plast Reconstr Surg Glob Open. 2022 Mar 25;10(3):e4271. doi: 10.1097/GOX.0000000000004271. eCollection 2022 Mar. Plast Reconstr Surg Glob Open. 2022. PMID: 35350147 Free PMC article.
Abstract
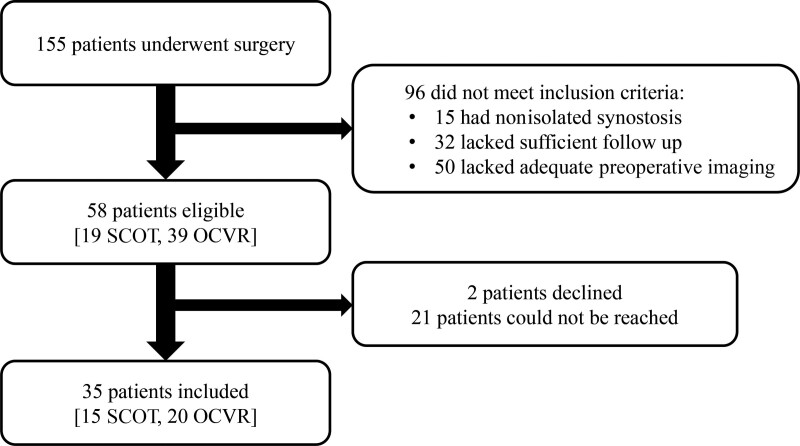
Background: Strip craniectomy with orthotic helmet therapy (SCOT) is an increasingly supported treatment for metopic craniosynostosis, although the long-term efficacy of deformity correction remains poorly defined. We compared the longterm outcomes of SCOT versus open cranial vault reconstruction (OCVR).
Methods: Patients who underwent OCVR or SCOT for isolated metopic synostosis with at least 3 years of follow-up were identified at our institution. Anthropometric measurements were used to assess baseline severity and postoperative skull morphology. Independent laypersons and craniofacial surgeons rated the appearance of each patient's 3D photographs, compared to normal controls.
Results: Thirty-five patients were included (15 SCOT and 20 OCVR), with similar follow-up between groups (SCOT 7.9 ± 3.2 years, OCVR 9.2 ± 4.1 years). Baseline severity and postoperative anthropometric measurements were equivalent. Independent adolescent raters reported that the forehead, eye, and overall appearance of SCOT patients was better than OCVR patients (P < 0.05, all comparisons). Craniofacial surgeons assigned Whitaker class I to a greater proportion of SCOT patients with moderate-to-severe synostosis (72.2 ± 5.6%) compared with OCVR patients with the same severity (33.3 ± 9.2%, P = 0.02). Parents of children who underwent SCOT reported equivalent satisfaction with the results of surgery (100% versus 95%, P > 0.99), and were no more likely to report bullying (7% versus 15%, P = 0.82).
Conclusions: SCOT was associated with superior long-term appearance and perioperative outcomes compared with OCVR. These findings suggest that SCOT should be the treatment of choice for patients with a timely diagnosis of metopic craniosynostosis.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Figures



References
-
- Dempsey RF, Monson LA, Maricevich RS, et al. Nonsyndromic craniosynostosis. Clin Plast Surg. 2019;46:123–139. - PubMed
-
- Fearon JA. Evidence-based medicine: craniosynostosis. Plast Reconstr Surg. 2014;133:1261–1275. - PubMed
-
- Jaskolka MS. Current controversies in metopic suture craniosynostosis. Oral Maxillofac Surg Clin North Am. 2017;29:447–463. - PubMed
-
- Kunz M, Lehner M, Heger A, et al. Neurodevelopmental and esthetic results in children after surgical correction of metopic suture synostosis: A single institutional experience. Childs Nerv Syst. 2014;30:1075–1082. - PubMed
LinkOut - more resources
Full Text Sources