

Clinical characteristics, risk factors and outcomes in patients with severe COVID-19 registered in the International Severe Acute Respiratory and Emerging Infection Consortium WHO clinical characterisation protocol: a prospective, multinational, multicentre, observational study
- PMID: 35169585
- PMCID: PMC8669808
- DOI: 10.1183/23120541.00552-2021
Clinical characteristics, risk factors and outcomes in patients with severe COVID-19 registered in the International Severe Acute Respiratory and Emerging Infection Consortium WHO clinical characterisation protocol: a prospective, multinational, multicentre, observational study
Abstract
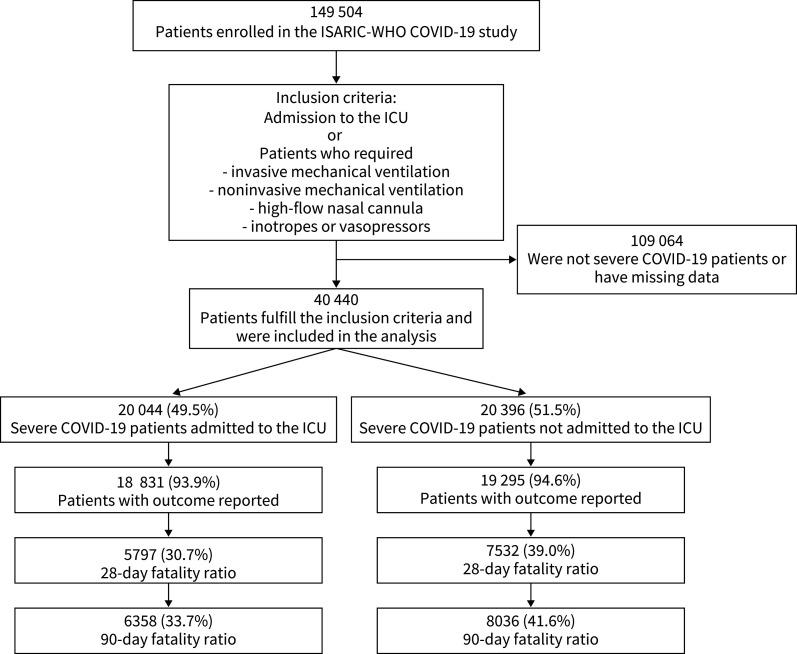
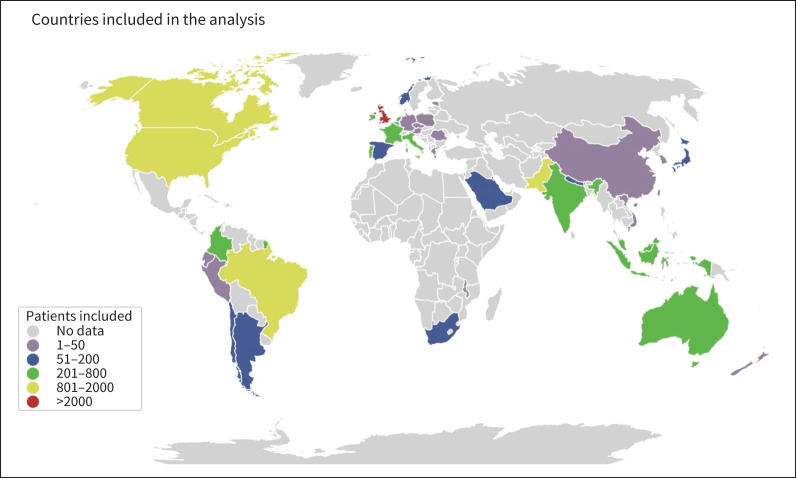
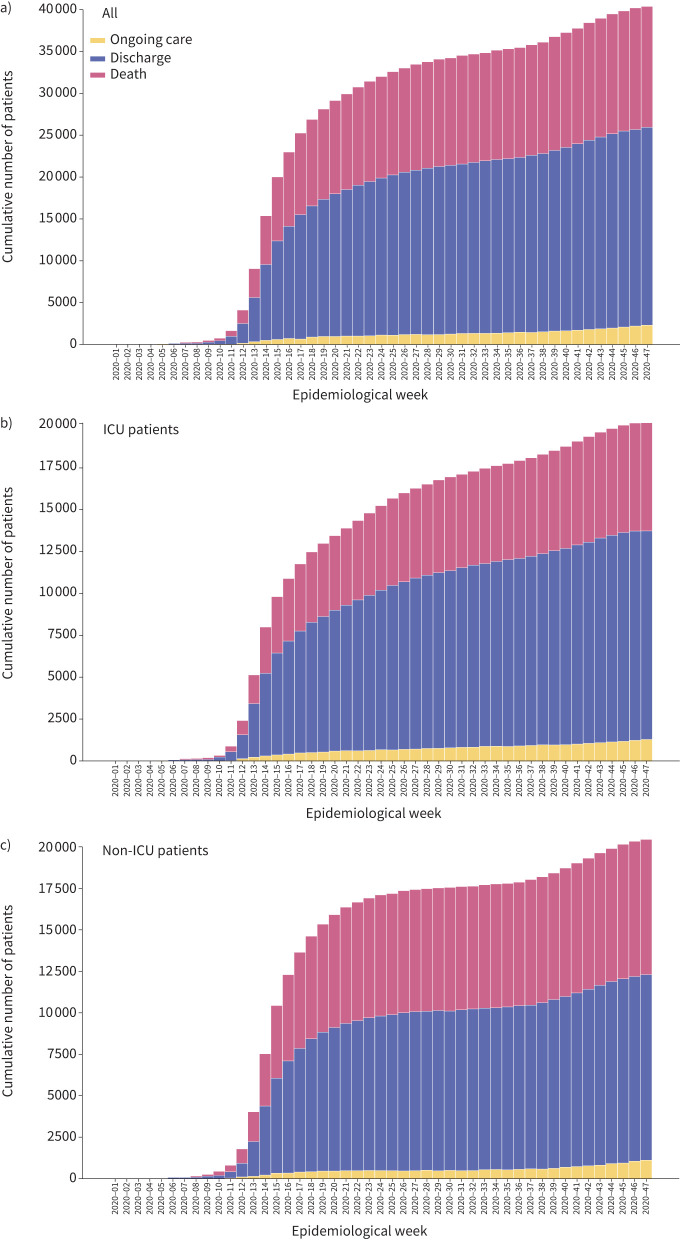
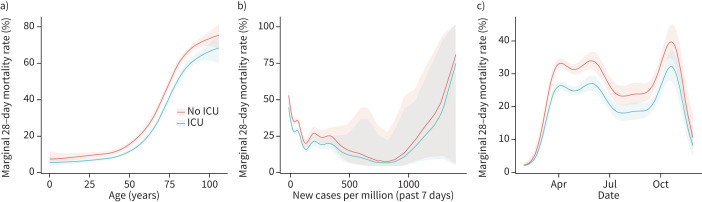
Due to the large number of patients with severe coronavirus disease 2019 (COVID-19), many were treated outside the traditional walls of the intensive care unit (ICU), and in many cases, by personnel who were not trained in critical care. The clinical characteristics and the relative impact of caring for severe COVID-19 patients outside the ICU is unknown. This was a multinational, multicentre, prospective cohort study embedded in the International Severe Acute Respiratory and Emerging Infection Consortium World Health Organization COVID-19 platform. Severe COVID-19 patients were identified as those admitted to an ICU and/or those treated with one of the following treatments: invasive or noninvasive mechanical ventilation, high-flow nasal cannula, inotropes or vasopressors. A logistic generalised additive model was used to compare clinical outcomes among patients admitted or not to the ICU. A total of 40 440 patients from 43 countries and six continents were included in this analysis. Severe COVID-19 patients were frequently male (62.9%), older adults (median (interquartile range (IQR), 67 (55-78) years), and with at least one comorbidity (63.2%). The overall median (IQR) length of hospital stay was 10 (5-19) days and was longer in patients admitted to an ICU than in those who were cared for outside the ICU (12 (6-23) days versus 8 (4-15) days, p<0.0001). The 28-day fatality ratio was lower in ICU-admitted patients (30.7% (5797 out of 18 831) versus 39.0% (7532 out of 19 295), p<0.0001). Patients admitted to an ICU had a significantly lower probability of death than those who were not (adjusted OR 0.70, 95% CI 0.65-0.75; p<0.0001). Patients with severe COVID-19 admitted to an ICU had significantly lower 28-day fatality ratio than those cared for outside an ICU.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: L.F. Reyes has nothing to disclose. Conflict of interest: S. Murthy declares receiving salary support from the Health Research Foundation and Innovative Medicines Canada Chair in Pandemic Preparedness Research. Conflict of interest: E. Garcia-Gallo has nothing to disclose. Conflict of interest: M. Irvine has nothing to disclose. Conflict of interest: L. Merson has nothing to disclose. Conflict of interest: I. Martin-Loeches declares consulting fees for Gilead outside of the submitted work. Conflict of interest: J. Rello has nothing to disclose. Conflict of interest: F.S. Taccone has nothing to disclose. Conflict of interest: R.A. Fowler has nothing to disclose. Conflict of interest: A.B. Docherty has nothing to disclose. Conflict of interest: C. Kartsonaki has nothing to disclose. Conflict of interest: I. Aragao has nothing to disclose. Conflict of interest: P.W. Barrett has nothing to disclose. Conflict of interest: A. Beane has nothing to disclose. Conflict of interest: A. Burrell has nothing to disclose. Conflict of interest: M.P. Cheng has nothing to disclose. Conflict of interest: M.D. Christian has nothing to disclose. Conflict of interest: J.P. Cidade has nothing to disclose. Conflict of interest: B.W. Citarella has nothing to disclose. Conflict of interest: C.A. Donnelly has nothing to disclose. Conflict of interest: S.M. Fernandes has nothing to disclose. Conflict of interest: C. French has nothing to disclose. Conflict of interest: R. Haniffa has nothing to disclose. Conflict of interest: E.M. Harrison has nothing to disclose. Conflict of interest: A.Y.W. Ho declares grant funding from Medical Research Council UK, Scottish Funding Council – Grand Challenges Research Fund and the Wellcome Trust, outside this submitted work. Conflict of interest: M. Joseph has nothing to disclose. Conflict of interest: I. Khan has nothing to disclose. Conflict of interest: M.E. Kho has nothing to disclose. Conflict of interest: A.B. Kildal has nothing to disclose. Conflict of interest: D. Kutsogiannis declares personal fees for a lecture from Tabuk Pharmaceuticals and the Saudi Critical Care Society. Conflict of interest: F. Lamontagne has nothing to disclose. Conflict of interest: T.C. Lee declares research salary support from les Fonds de recherche du Québec – Santé. Conflict of interest: G.L. Bassi has nothing to disclose. Conflict of interest: J.W. Lopez Revilla has nothing to disclose. Conflict of interest: C. Marquis has nothing to disclose. Conflict of interest: J. Millar has nothing to disclose. Conflict of interest: R. Neto has nothing to disclose. Conflict of interest: A. Nichol declares a grant from the Health Research Board of Ireland to support data collection in Ireland (CTN-2014-012). Conflict of interest: R. Parke has nothing to disclose. Conflict of interest: R. Pereira has nothing to disclose. Conflict of interest: S. Poli has nothing to disclose. Conflict of interest: P. Povoa declares personal fees (for lectures and advisory boards) from MSD, Technophage, Sanofi and Gilead. Conflict of interest: K. Ramanathan has nothing to disclose. Conflict of interest: O. Rewa declares consulting fees from Baxter Inc. Conflict of interest: J. Riera has nothing to disclose. Conflict of interest: S. Shrapnel participated as an investigator for an observational study analysing intensive care unit patients with COVID-19 (for the Critical Care Consortium including ECMOCARD) funded by The Prince Charles Hospital Foundation during the conduct of this study. S. Shrapnel reports in kind support from the Australian Research Council Centre of Excellence for Engineered Quantum Systems (CE170100009). Conflict of interest: M.J. Silva has nothing to disclose. Conflict of interest: A. Udy has nothing to disclose. Conflict of interest: T. Uyeki has nothing to disclose. Conflict of interest: S.A. Webb has nothing to disclose. Conflict of interest: E-J. Wils has nothing to disclose. Conflict of interest: A. Rojek has nothing to disclose. Conflict of interest: P.L. Olliaro has nothing to disclose.
Figures
References
-
- Rodríguez A, Ruiz-Botella M, Martín-Loeches I, et al. Deploying unsupervised clustering analysis to derive clinical phenotypes and risk factors associated with mortality risk in 2022 critically ill patients with COVID-19 in Spain. Crit Care 2021; 25: 63. doi: 10.1186/s13054-021-03487-8 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources