

Which children and young people are at higher risk of severe disease and death after hospitalisation with SARS-CoV-2 infection in children and young people: A systematic review and individual patient meta-analysis
- PMID: 35169689
- PMCID: PMC8832134
- DOI: 10.1016/j.eclinm.2022.101287
Which children and young people are at higher risk of severe disease and death after hospitalisation with SARS-CoV-2 infection in children and young people: A systematic review and individual patient meta-analysis
Abstract
Background: We aimed to describe pre-existing factors associated with severe disease, primarily admission to critical care, and death secondary to SARS-CoV-2 infection in hospitalised children and young people (CYP), within a systematic review and individual patient meta-analysis.
Methods: We searched Pubmed, European PMC, Medline and Embase for case series and cohort studies published between 1st January 2020 and 21st May 2021 which included all CYP admitted to hospital with ≥ 30 CYP with SARS-CoV-2 or ≥ 5 CYP with PIMS-TS or MIS-C. Eligible studies contained (1) details of age, sex, ethnicity or co-morbidities, and (2) an outcome which included admission to critical care, mechanical invasive ventilation, cardiovascular support, or death. Studies reporting outcomes in more restricted groupings of co-morbidities were eligible for narrative review. We used random effects meta-analyses for aggregate study-level data and multilevel mixed effect models for IPD data to examine risk factors (age, sex, comorbidities) associated with admission to critical care and death. Data shown are odds ratios and 95% confidence intervals (CI).PROSPERO: CRD42021235338.
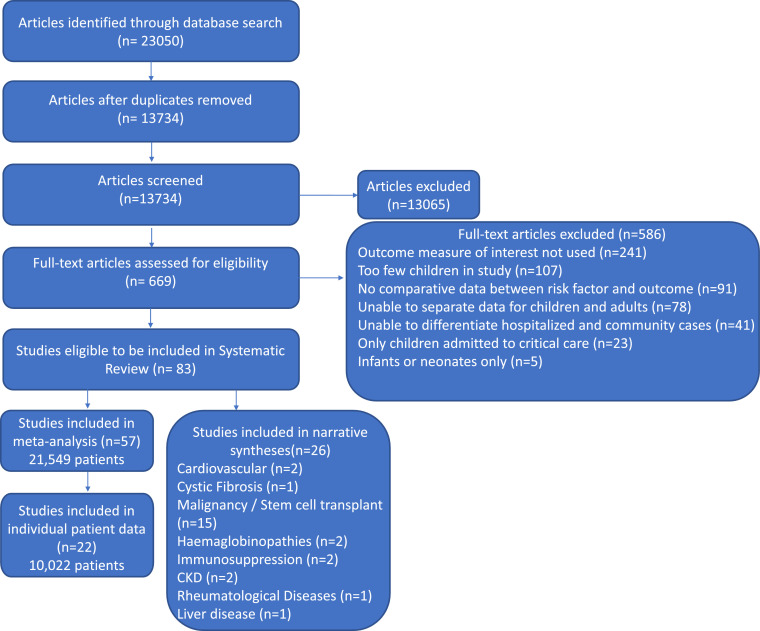
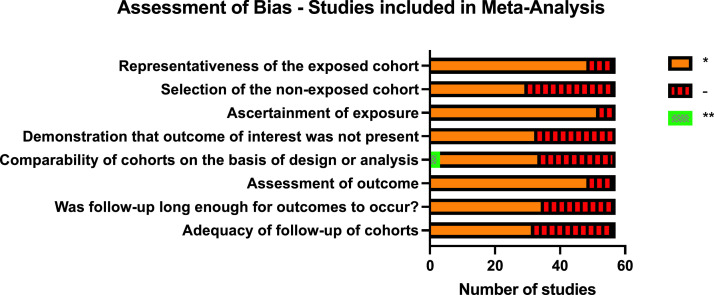
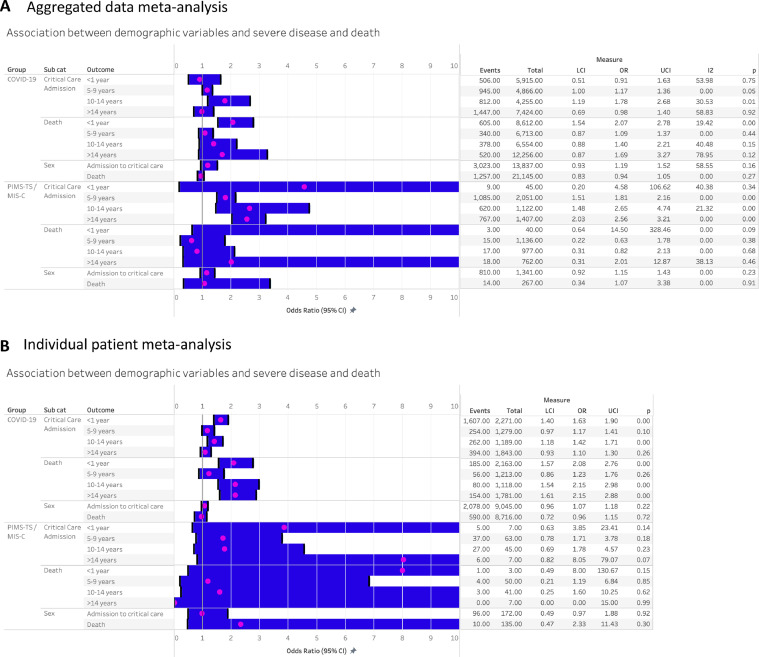
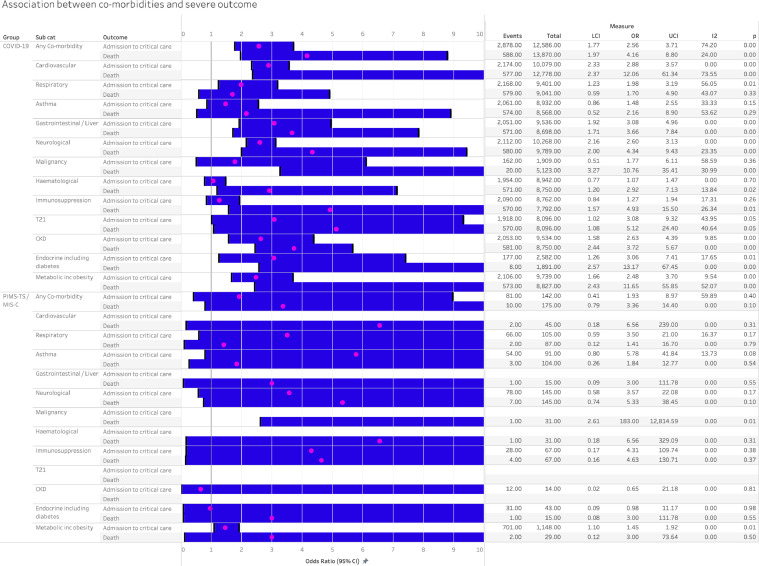
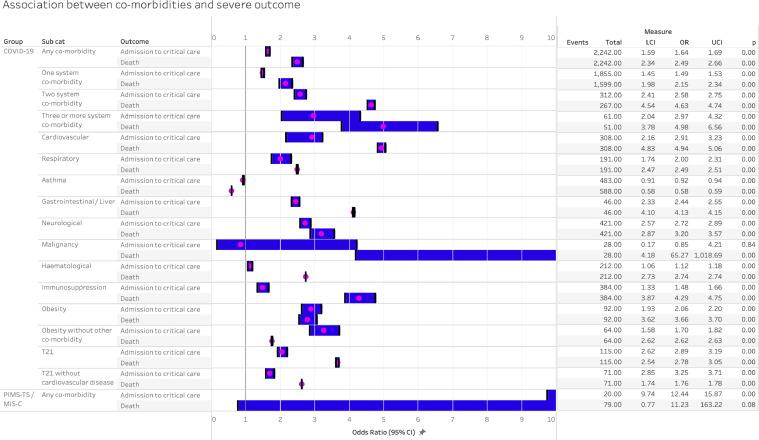
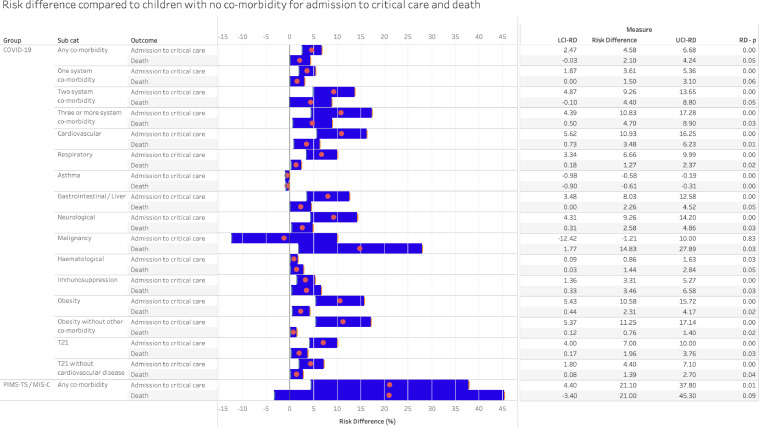
Findings: 83 studies were included, 57 (21,549 patients) in the meta-analysis (of which 22 provided IPD) and 26 in the narrative synthesis. Most studies had an element of bias in their design or reporting. Sex was not associated with critical care or death. Compared with CYP aged 1-4 years (reference group), infants (aged <1 year) had increased odds of admission to critical care (OR 1.63 (95% CI 1.40-1.90)) and death (OR 2.08 (1.57-2.86)). Odds of death were increased amongst CYP over 10 years (10-14 years OR 2.15 (1.54-2.98); >14 years OR 2.15 (1.61-2.88)).The number of comorbid conditions was associated with increased odds of admission to critical care and death for COVID-19 in a step-wise fashion. Compared with CYP without comorbidity, odds ratios for critical care admission were: 1.49 (1.45-1.53) for 1 comorbidity; 2.58 (2.41-2.75) for 2 comorbidities; 2.97 (2.04-4.32) for ≥3 comorbidities. Corresponding odds ratios for death were: 2.15 (1.98-2.34) for 1 comorbidity; 4.63 (4.54-4.74) for 2 comorbidities and 4.98 (3.78-6.65) for ≥3 comorbidities. Odds of admission to critical care were increased for all co-morbidities apart from asthma (0.92 (0.91-0.94)) and malignancy (0.85 (0.17-4.21)) with an increased odds of death in all co-morbidities considered apart from asthma. Neurological and cardiac comorbidities were associated with the greatest increase in odds of severe disease or death. Obesity increased the odds of severe disease and death independently of other comorbidities. IPD analysis demonstrated that, compared to children without co-morbidity, the risk difference of admission to critical care was increased in those with 1 comorbidity by 3.61% (1.87-5.36); 2 comorbidities by 9.26% (4.87-13.65); ≥3 comorbidities 10.83% (4.39-17.28), and for death: 1 comorbidity 1.50% (0.00-3.10); 2 comorbidities 4.40% (-0.10-8.80) and ≥3 co-morbidities 4.70 (0.50-8.90).
Interpretation: Hospitalised CYP at greatest vulnerability of severe disease or death with SARS-CoV-2 infection are infants, teenagers, those with cardiac or neurological conditions, or 2 or more comorbid conditions, and those who are obese. These groups should be considered higher priority for vaccination and for protective shielding when appropriate. Whilst odds ratios were high, the absolute increase in risk for most comorbidities was small compared to children without underlying conditions.
Funding: RH is in receipt of a fellowship from Kidney Research UK (grant no. TF_010_20171124). JW is in receipt of a Medical Research Council Fellowship (Grant No. MR/R00160X/1). LF is in receipt of funding from Martin House Children's Hospice (there is no specific grant number for this). RV is in receipt of a grant from the National Institute of Health Research to support this work (grant no NIHR202322). Funders had no role in study design, data collection, analysis, decision to publish or preparation of the manuscript.
Keywords: Adolescent; COVID-19; Child; Chronic condition; Hospitalisation; Intensive care; Meta-analysis; Mortality; Risk factor; SARS-CoV-2; Severity; Systematic review.
© 2022 The Authors.
Conflict of interest statement
KL is the Programme Lead for the National Child Mortality Database. SK is the National Clinical Director for Children and Young People, NHS England and Improvement. ED is the Co-Principle Investigator for the Paediatric Intensive Care Audit Network.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
