

Towards guided and automated programming of subthalamic area stimulation in Parkinson's disease
- PMID: 35169708
- PMCID: PMC8833293
- DOI: 10.1093/braincomms/fcac003
Towards guided and automated programming of subthalamic area stimulation in Parkinson's disease
Abstract
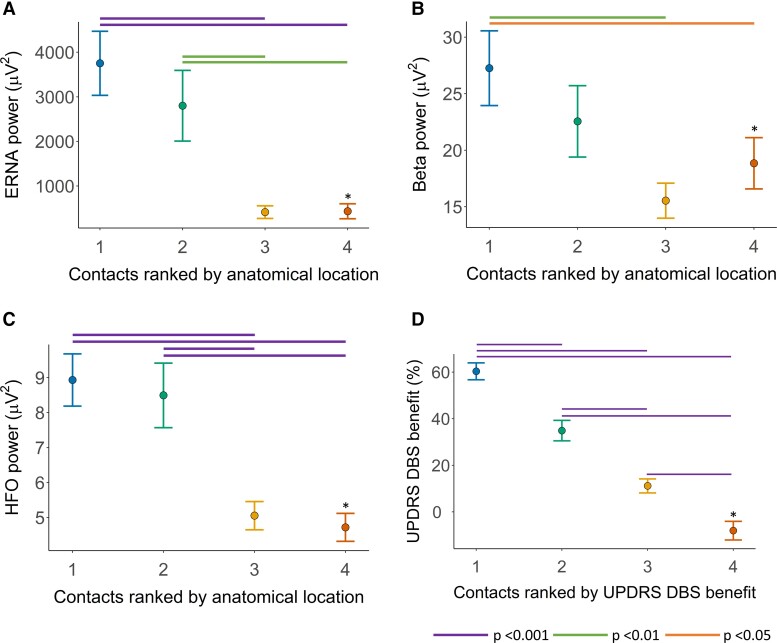
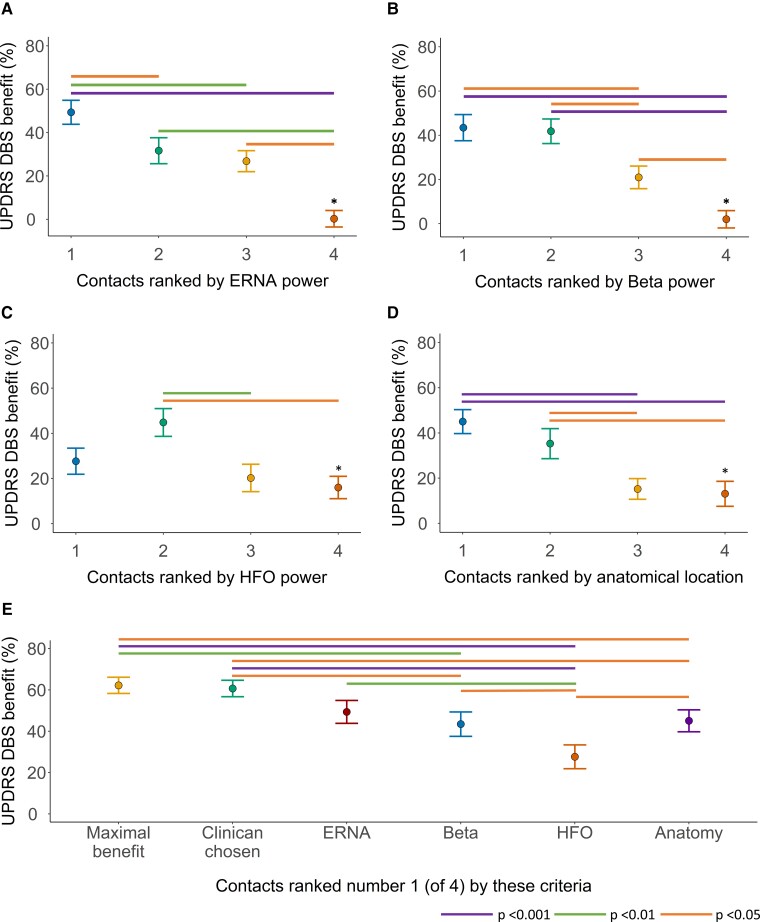
Selecting the ideal contact to apply subthalamic nucleus deep brain stimulation in Parkinson's disease can be an arduous process, with outcomes highly dependent on clinician expertise. This study aims to assess whether neuronal signals recorded intraoperatively in awake patients, and the anatomical location of contacts, can assist programming. In a cohort of 14 patients with Parkinson's disease, implanted with subthalamic nucleus deep brain stimulation, the four contacts on each lead in the 28 hemispheres were ranked according to proximity to a nominated ideal anatomical location and power of the following neuronal signals: evoked resonant neural activity, beta oscillations and high-frequency oscillations. We assessed how these rankings predicted, on each lead: (i) the motor benefit from deep brain stimulation applied through each contact and (ii) the 'ideal' contact to apply deep brain stimulation. The ranking of contacts according to each factor predicted motor benefit from subthalamic nucleus deep brain stimulation, as follows: evoked resonant neural activity; r 2 = 0.50, Akaike information criterion 1039.9, beta; r 2 = 0.50, Akaike information criterion 1041.6, high-frequency oscillations; r 2 = 0.44, Akaike information criterion 1057.2 and anatomy; r 2 = 0.49, Akaike information criterion 1048.0. Combining evoked resonant neural activity, beta and high-frequency oscillations ranking data yielded the strongest predictive model (r 2 = 0.61, Akaike information criterion 1021.5). The 'ideal' contact (yielding maximal benefit) was ranked first according to each factor in the following proportion of hemispheres; evoked resonant neural activity 18/28, beta 17/28, anatomy 16/28, high-frequency oscillations 7/28. Across hemispheres, the maximal available deep brain stimulation benefit did not differ from that yielded by contacts chosen by clinicians for chronic therapy or contacts ranked first according to evoked resonant neural activity. Evoked resonant neural activity, beta oscillations and anatomy similarly predicted how motor benefit from subthalamic nucleus deep brain stimulation varied across contacts on each lead. This could assist programming by providing a probability ranking of contacts akin to a 'monopolar survey'. However, these factors identified the 'ideal' contact in only a proportion of hemispheres. More advanced signal processing and anatomical techniques may be needed for the full automation of contact selection.
Keywords: Parkinson’s disease; deep brain stimulation; evoked potentials; local field potentials; subthalamic nucleus.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures



References
-
- Volkmann J, Moro E, Pahwa R. Basic algorithms for the programming of deep brain stimulation in Parkinson’s disease. Mov Disord. 2006;21(S14):S284–S289. - PubMed
-
- Picillo M, Lozano AM, Kou N, Munhoz RP, Fasano A. Programming deep brain stimulation for Parkinson’s disease: The Toronto western hospital algorithms. Brain Stimulat. 2016;9(3):425–437. - PubMed
-
- Temperli P, Ghika J, Villemure J-G, Burkhard PR, Bogousslavsky J, Vingerhoets FJ. How do parkinsonian signs return after discontinuation of subthalamic DBS? Neurology. 2003;60(1):78–81. - PubMed
-
- Mestre TA, Lang AE, Okun MS. Factors influencing the outcome of deep brain stimulation: Placebo, nocebo, lessebo, and lesion effects. Mov Disord. 2016;31(3):290–298. - PubMed
-
- Okun MS, Tagliati M, Pourfar M, et al. Management of referred deep brain stimulation failures: A retrospective analysis from 2 movement disorders centers. Arch Neurol. 2005;62(8):1250–1255. - PubMed
LinkOut - more resources
Full Text Sources