

Surgical management of diastolic heart failure after septal myectomy for obstructive hypertrophic cardiomyopathy
- PMID: 35169725
- PMCID: PMC8828785
- DOI: 10.1016/j.xjtc.2021.10.050
Surgical management of diastolic heart failure after septal myectomy for obstructive hypertrophic cardiomyopathy
Abstract
Objective: Some patients with obstructive hypertrophic cardiomyopathy may remain limited after surgical relief of the subaortic obstruction. In this report, we describe experience in surgical management of patients with advanced diastolic heart failure symptoms after adequate transaortic septal myectomy for obstructive hypertrophic cardiomyopathy.
Methods: We identified adult patients who presented with heart failure symptoms after previous transaortic septal myectomy for obstructive hypertrophic cardiomyopathy and underwent repeat sternotomy for transapical myectomy to enlarge a small left ventricular cavity. Functional recovery after hospital dismissal was assessed through a questionnaire-based survey.
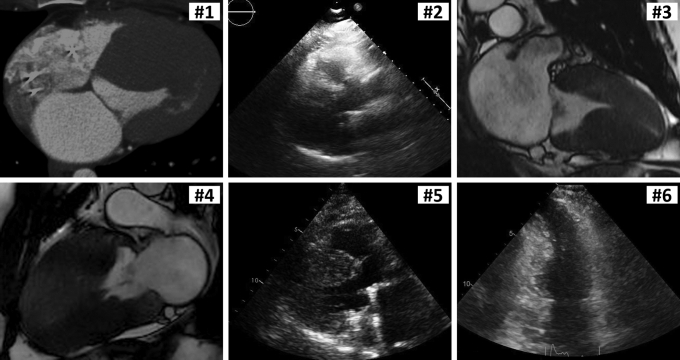
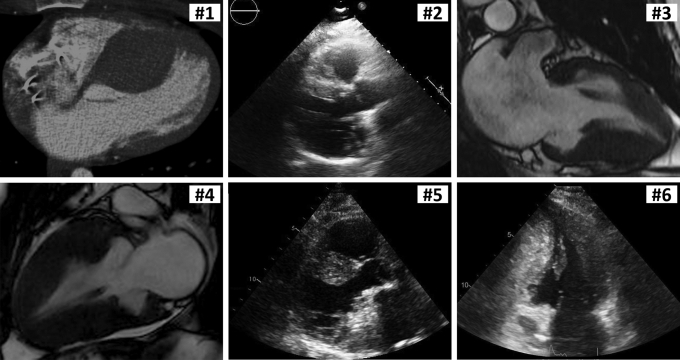
Results: Six patients with previous septal myectomy presented with New York Heart Association functional class III symptoms. Preoperative transthoracic Doppler echocardiography confirmed adequate relief of subaortic outflow tract obstruction with only trivial or mild mitral valve regurgitation; left atrial volume index was increased at 46 mL/m2 (range, 44-47 mL/m2). Following transapical myectomy, the left ventricular diameter was enlarged from 23 mm (range, 21-27 mm) to 29 mm (range, 27-31 mm) at end-systole and from 40 mm (range, 38-42 mm) to 43 mm (range, 42-50 mm) at end-diastole. All the patients were alive after a median follow-up of 0.6 years (range, 0.4-3.5 years), and 5 patients responded to a postoperative survey and indicated improvement in their heart condition compared with functional status before the repeat myectomy.
Conclusions: Patients with diastolic heart failure after septal myectomy for obstructive hypertrophic cardiomyopathy may present with systolic cavity obliteration due to excessive myocardial hypertrophy. Repeat transapical myectomy can enlarge the left ventricular chamber and augment the diastolic volume, which results in improved physical capacity and patient-perceived functional status.
Keywords: AF, atrial fibrillation; EF, ejection fraction; HCM, hypertrophic cardiomyopathy; LV, left ventricular; LVOT, left ventricular outflow tract; TTE, transthoracic echocardiography; diastolic heart failure; hypertrophic cardiomyopathy; repeat operation; transapical myectomy.
© 2021 The Author(s).
Figures

References
-
- Maron M.S., Olivotto I., Zenovich A.G., Link M.S., Pandian N.G., Kuvin J.T., et al. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114:2232–2239. - PubMed
-
- Wells S., Rowin E.J., Boll G., Rastegar H., Wang W., Maron M.S., et al. Clinical profile of nonresponders to surgical myectomy with obstructive hypertrophic cardiomyopathy. Am J Med. 2018;131:e235–e239. - PubMed
-
- Nishimura R.A., Seggewiss H., Schaff H.V. Hypertrophic obstructive cardiomyopathy: surgical myectomy and septal ablation. Circ Res. 2017;121:771–783. - PubMed
-
- Yacoub M.H., Olivotto I., Cecchi F. “End-stage” hypertrophic cardiomyopathy: from mystery to model. Nat Clin Pract Cardiovasc Med. 2007;4:232–233. - PubMed
LinkOut - more resources
Full Text Sources
