

Prevalence of statin intolerance: a meta-analysis
- PMID: 35169843
- PMCID: PMC9757867
- DOI: 10.1093/eurheartj/ehac015
Prevalence of statin intolerance: a meta-analysis
Abstract
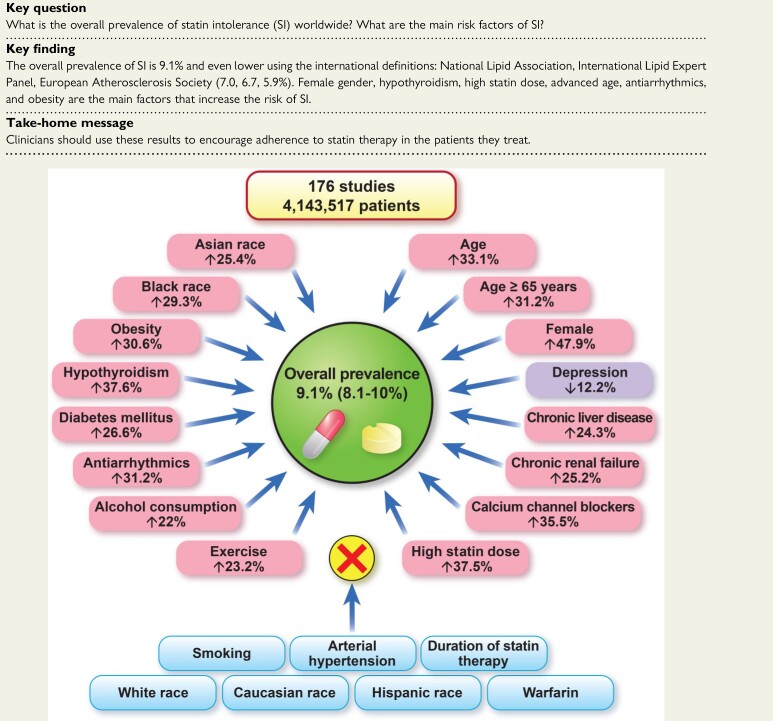
Aims: Statin intolerance (SI) represents a significant public health problem for which precise estimates of prevalence are needed. Statin intolerance remains an important clinical challenge, and it is associated with an increased risk of cardiovascular events. This meta-analysis estimates the overall prevalence of SI, the prevalence according to different diagnostic criteria and in different disease settings, and identifies possible risk factors/conditions that might increase the risk of SI.
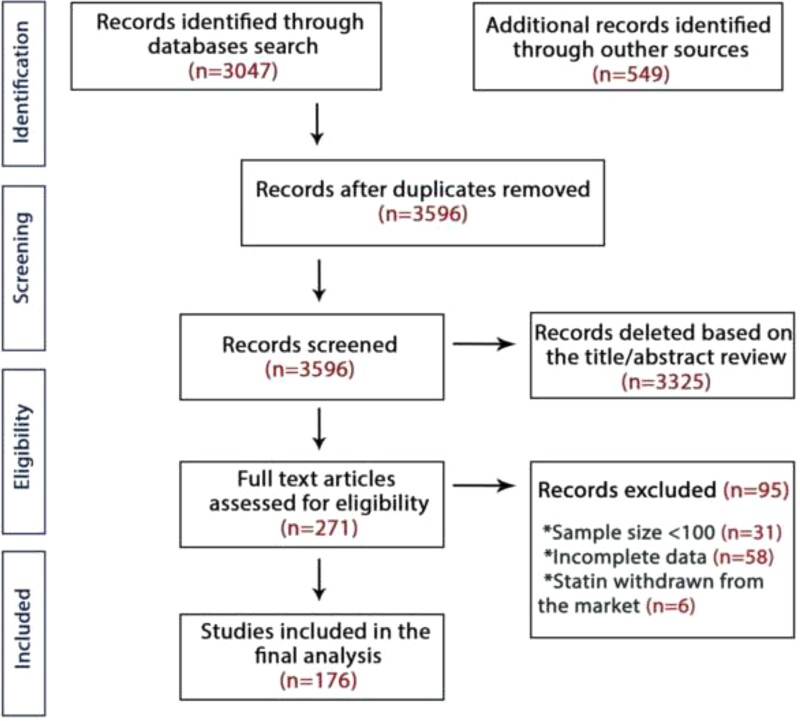
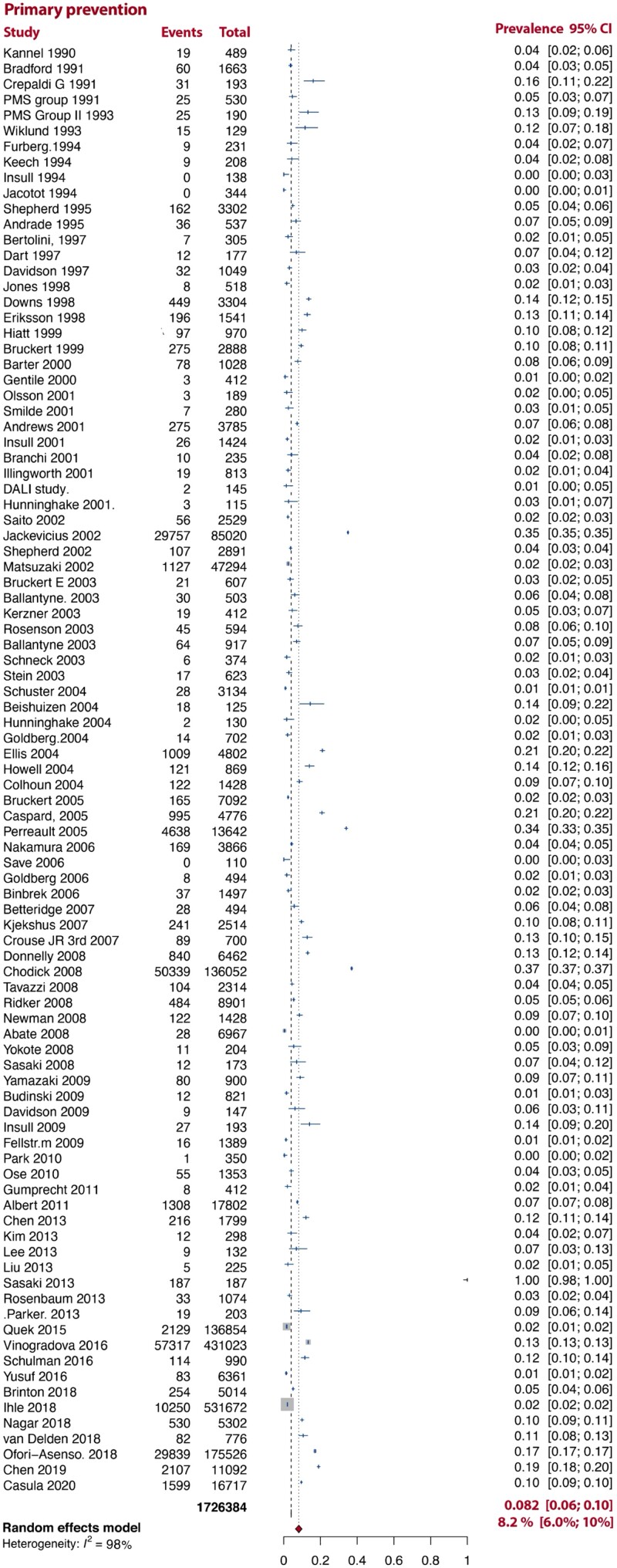
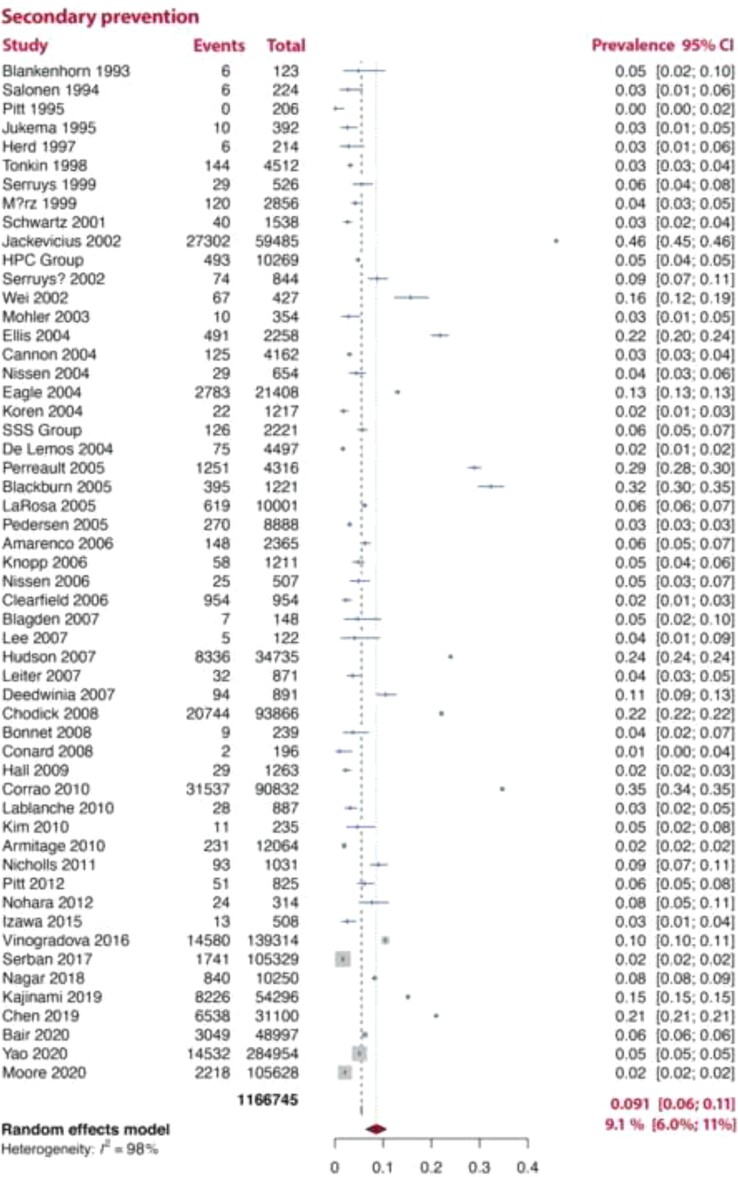
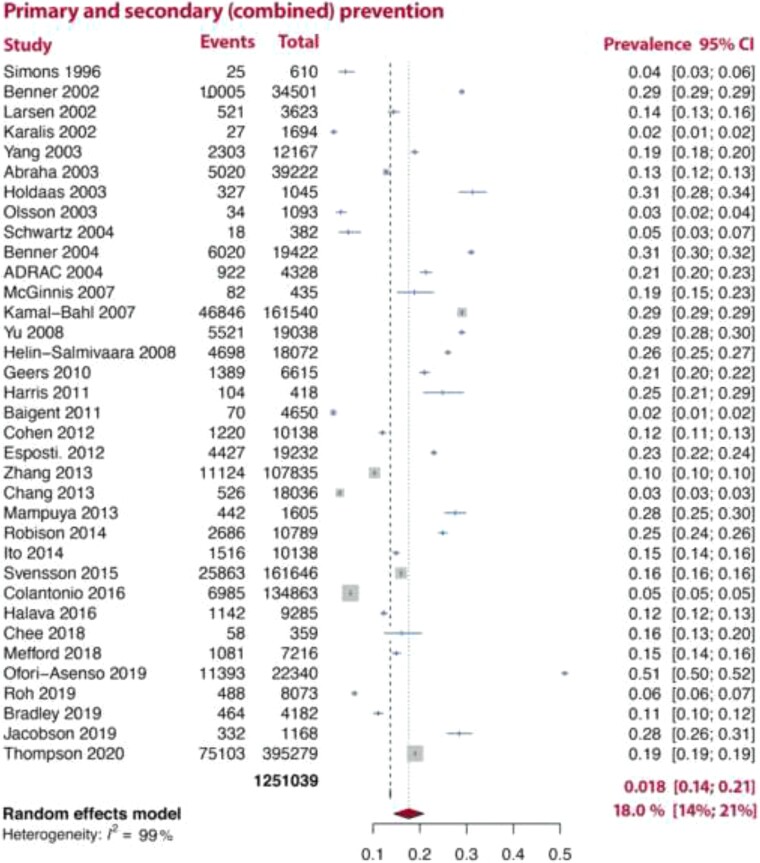
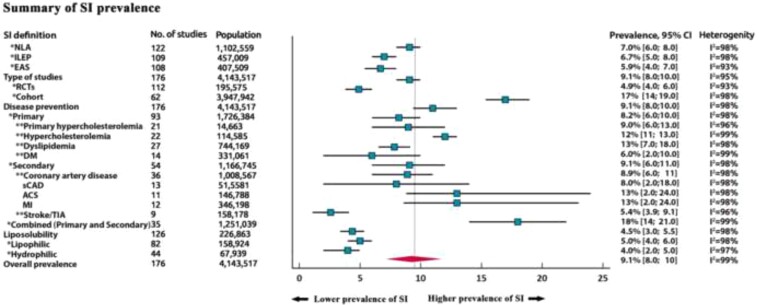
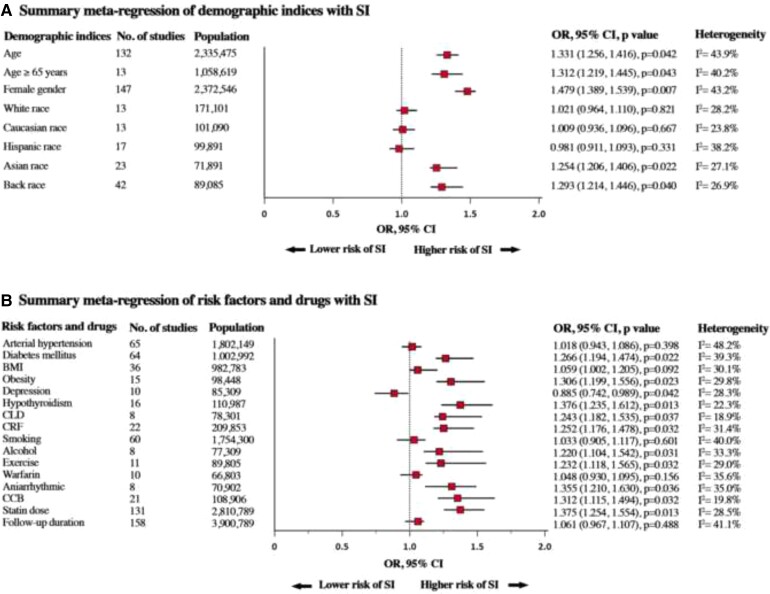
Methods and results: We searched several databases up to 31 May 2021, for studies that reported the prevalence of SI. The primary endpoint was overall prevalence and prevalence according to a range of diagnostic criteria [National Lipid Association (NLA), International Lipid Expert Panel (ILEP), and European Atherosclerosis Society (EAS)] and in different disease settings. The secondary endpoint was to identify possible risk factors for SI. A random-effects model was applied to estimate the overall pooled prevalence. A total of 176 studies [112 randomized controlled trials (RCTs); 64 cohort studies] with 4 143 517 patients were ultimately included in the analysis. The overall prevalence of SI was 9.1% (95% confidence interval 8.0-10%). The prevalence was similar when defined using NLA, ILEP, and EAS criteria [7.0% (6.0-8.0%), 6.7% (5.0-8.0%), 5.9% (4.0-7.0%), respectively]. The prevalence of SI in RCTs was significantly lower compared with cohort studies [4.9% (4.0-6.0%) vs. 17% (14-19%)]. The prevalence of SI in studies including both primary and secondary prevention patients was much higher than when primary or secondary prevention patients were analysed separately [18% (14-21%), 8.2% (6.0-10%), 9.1% (6.0-11%), respectively]. Statin lipid solubility did not affect the prevalence of SI [4.0% (2.0-5.0%) vs. 5.0% (4.0-6.0%)]. Age [odds ratio (OR) 1.33, P = 0.04], female gender (OR 1.47, P = 0.007), Asian and Black race (P < 0.05 for both), obesity (OR 1.30, P = 0.02), diabetes mellitus (OR 1.26, P = 0.02), hypothyroidism (OR 1.37, P = 0.01), chronic liver, and renal failure (P < 0.05 for both) were significantly associated with SI in the meta-regression model. Antiarrhythmic agents, calcium channel blockers, alcohol use, and increased statin dose were also associated with a higher risk of SI.
Conclusion: Based on the present analysis of >4 million patients, the prevalence of SI is low when diagnosed according to international definitions. These results support the concept that the prevalence of complete SI might often be overestimated and highlight the need for the careful assessment of patients with potential symptoms related to SI.
Keywords: Cardiovascular disease; Prevalence; Risk factors; Statin intolerance.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: P.E.P. has received honoraria and/or travel reimbursement for events sponsored by AKCEA, Amgen, AMRYT, Link Medical, Mylan, Napp, Sanofi; D.P.M. has given talks, acted as a consultant, or attended conferences sponsored by Amgen and Novo Nordisk; P.P.T.: speaker for Amgen, Esperion, Merck, Novo Nordisk; consultant to Amarin, Amgen, Kowa, Merck, Resverlogix, and Theravance; Ž.R. has given talks sponsored by Sanofi-Aventis and Novartis; M.B.: speakers bureau: Amgen, Herbapol, Kogen, KRKA, Polpharma, Mylan/Viatris, Novartis, Novo Nordisk, Sanofi-Aventis, Teva, Zentiva; consultant to Abbott Vascular, Amgen, Daichii Sankyo, Esperion, FreiaPharmaceuticals, Novartis, Polfarmex, Sanofi-Aventis; Grants from Amgen, Mylan/Viatris, Sanofi, and Valeant; CMO at Nomi Biotech Corporation; all other authors have no conflict of interest.
Figures
Comment in
-
Statin intolerance: how common is it and how do we work with patients to overcome it?Eur Heart J. 2022 Sep 7;43(34):3224-3226. doi: 10.1093/eurheartj/ehac156. Eur Heart J. 2022. PMID: 35325103 No abstract available.
References
-
- Stone NJ, Robinson J, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2889–2934. - PubMed
-
- Banach M, Stulc T, Dent R, Toth PP. Statin non-adherence and residual cardiovascular risk: there is need for substantial improvement. Int J Cardiol 2016;225:184–196. - PubMed
-
- Rosenson RS, Baker S, Banach M, Borow KM, Braun LT, Bruckert E, et al. Optimizing cholesterol treatment in patients with muscle complaints. J Am Coll Cardiol 2017;70:1290–1301. - PubMed
