

FGFR2::TACC2 fusion as a novel KIT-independent mechanism of targeted therapy failure in a multidrug-resistant gastrointestinal stromal tumor
- PMID: 35170141
- PMCID: PMC9194600
- DOI: 10.1002/gcc.23030
FGFR2::TACC2 fusion as a novel KIT-independent mechanism of targeted therapy failure in a multidrug-resistant gastrointestinal stromal tumor
Abstract
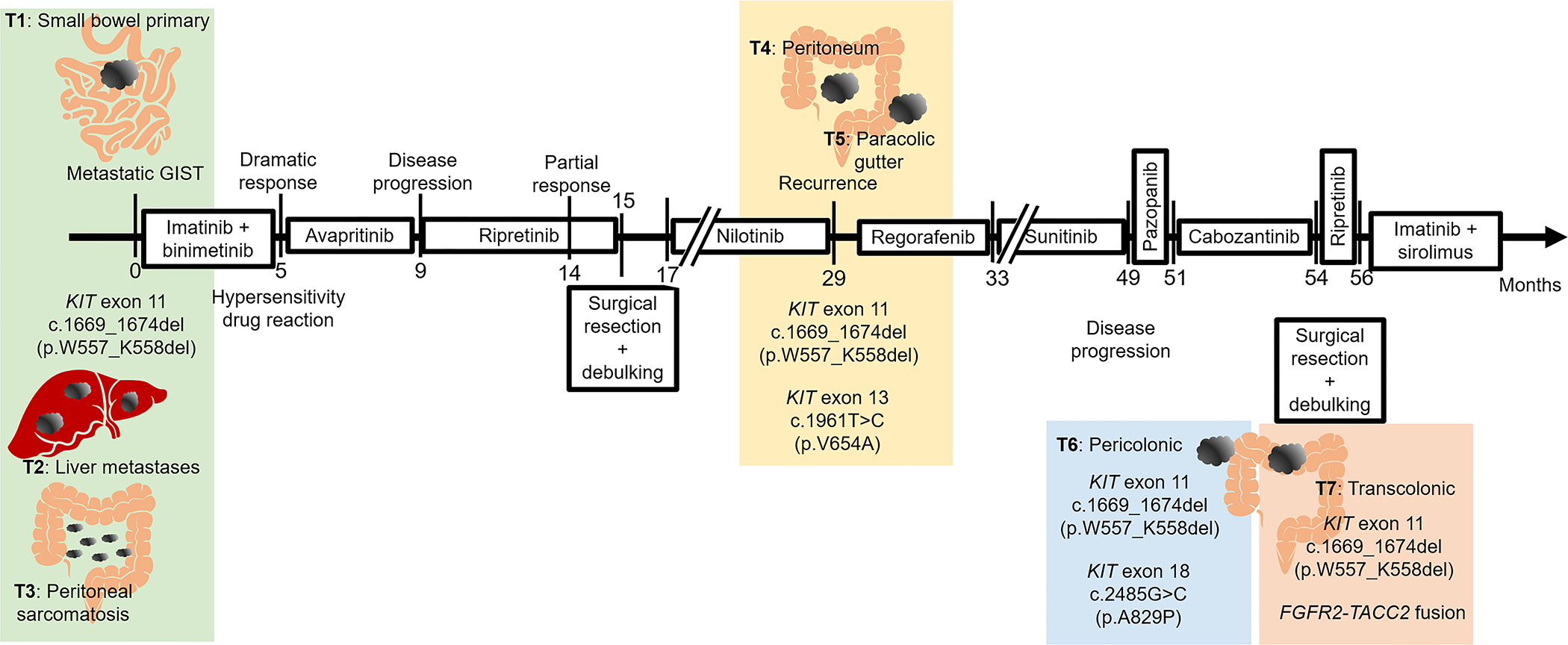
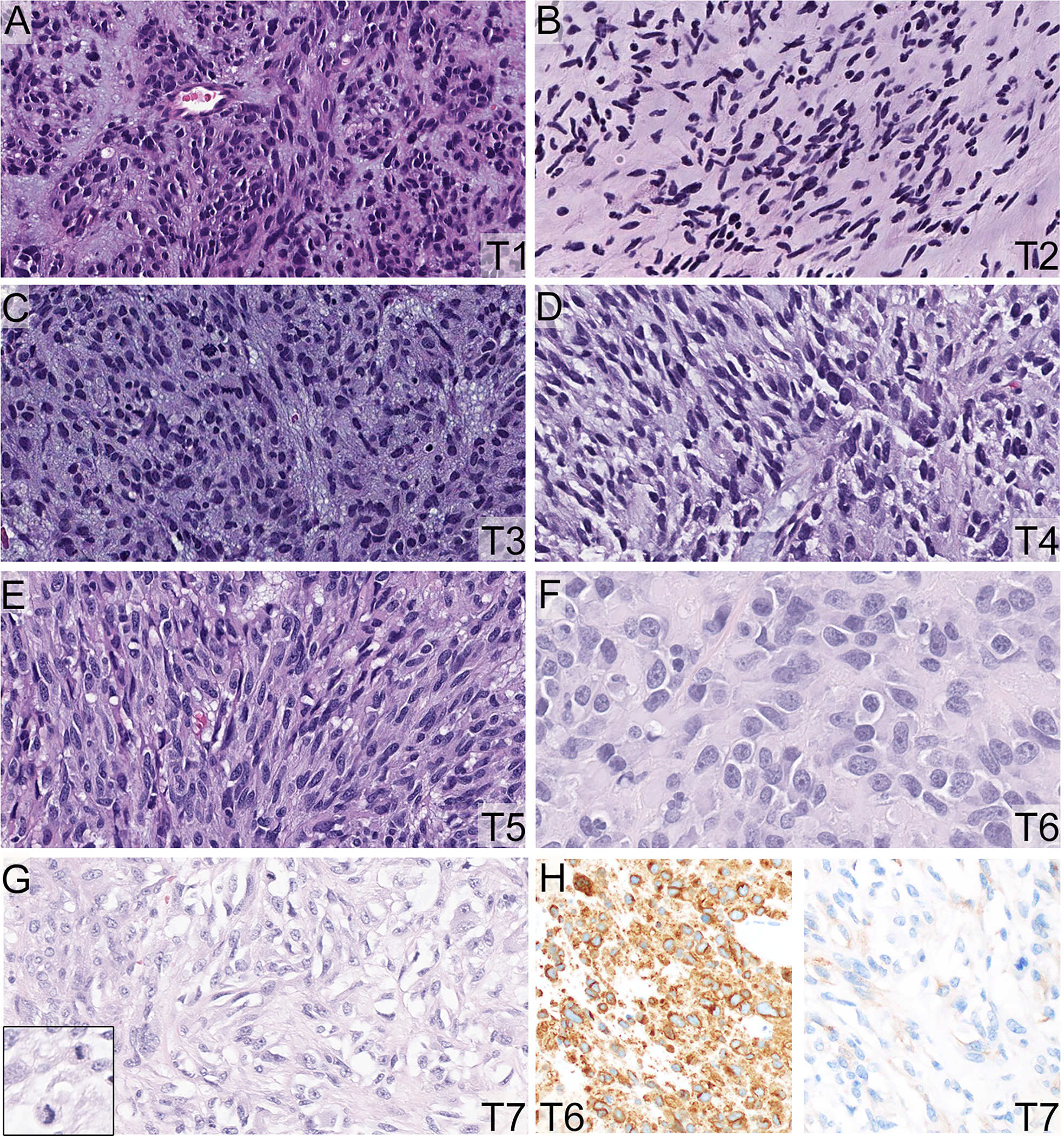
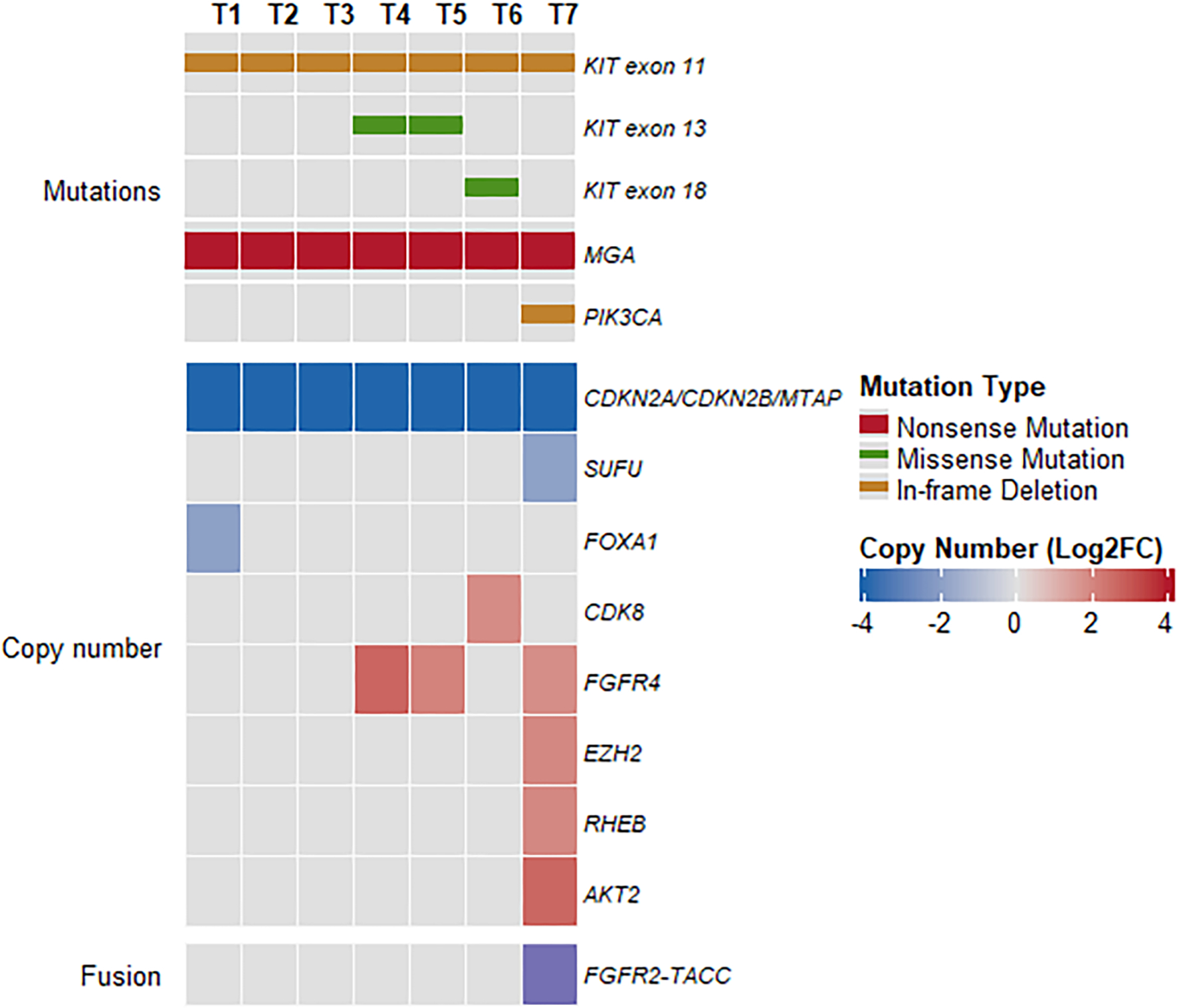
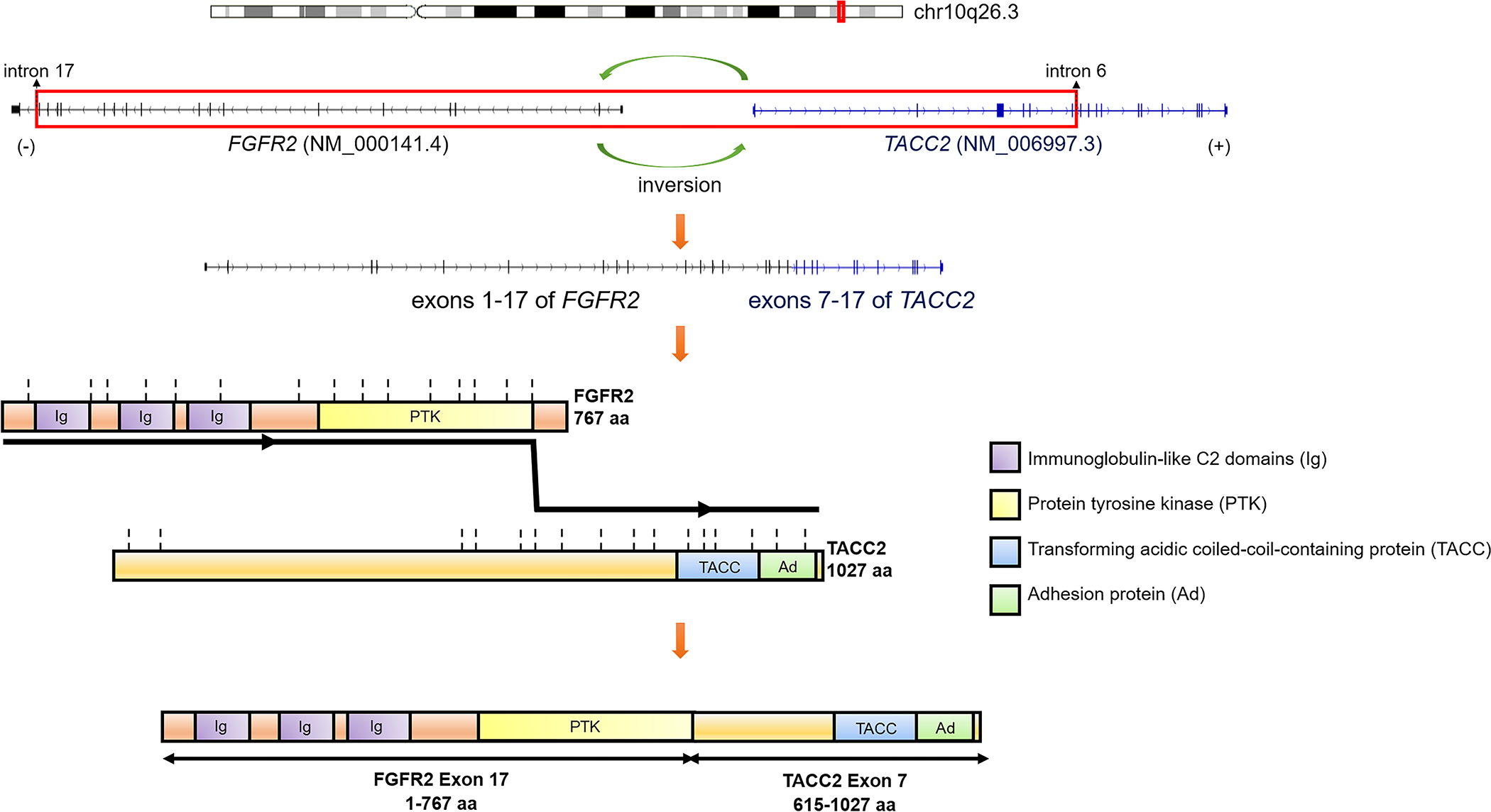
Genetic alterations in FGF/FGFR pathway are infrequent in gastrointestinal stromal tumors (GIST), with rare cases of quadruple wildtype GISTs harboring FGFR1 gene fusions and mutations. Additionally, FGF/FGFR overexpression was shown to promote drug resistance to kinase inhibitors in GISTs. However, FGFR gene fusions have not been directly implicated as a mechanism of drug resistance in GISTs. Herein, we report a patient presenting with a primary small bowel spindle cell GIST and concurrent peritoneal and liver metastases displaying an imatinib-sensitive KIT exon 11 in-frame deletion. After an initial 9-month benefit to imatinib, the patient experienced intraabdominal peritoneal recurrence owing to secondary KIT exon 13 missense mutation and FGFR4 amplification. Despite several additional rounds of tyrosine kinase inhibitors (TKI), the patient's disease progressed after 2 years and presented with multiple peritoneal and liver metastases, including one pericolonic mass harboring secondary KIT exon 18 missense mutation, and a concurrent transverse colonic mass with a FGFR2::TACC2 fusion and AKT2 amplification. All tumors, including primary and recurrent masses, harbored an MGA c.7272 T > G (p.Y2424*) nonsense mutation and CDKN2A/CDKN2B/MTAP deletions. The transcolonic mass showed elevated mitotic count (18/10 HPF), as well as significant decrease in CD117 and DOG1 expression, in contrast to all the other resistant nodules that displayed diffuse and strong CD117 and DOG1 immunostaining. The FGFR2::TACC2 fusion resulted from a 742 kb intrachromosomal inversion at the chr10q26.3 locus, leading to a fusion between exons 1-17 of FGFR2 and exons 7-17 TACC2, which preserves the extracellular and protein tyrosine kinase domains of FGFR2. We present the first report of a multidrug-resistant GIST patient who developed an FGFR2 gene fusion as a secondary genetic event to the selective pressure of various TKIs. This case also highlights the heterogeneous escape mechanisms to targeted therapy across various tumor nodules, spanning from both KIT-dependent and KIT-independent off-target activation pathways.
Keywords: FGFR2; KIT; TKI; drug resistance; gastrointestinal stromal tumor; gene fusion.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
Conflict of Interest Disclosures
WT reports personal fees from Eli Lilly, EMD Serono, Mundipharma, C4 Therapeutics, Daiichi Sankyo, Blueprint, Agios Pharmaceuticals, NanoCarrier, Deciphera, Adcendo, Ayala Pharmaceuticals, Kowa, Servier, Bayer Pharmaceuticals, Epizyme, Cogent, Medpacto, Foghorn Therapeutics. In addition, WT holds patents in companion diagnostics for CDK4 inhibitors. He serves on the Scientific Advisory Board for Certis Oncology Solutions and Innova Therapeutics. He reports stock ownership for Atropos Therapeutics, and Innova Therapeutics.
Figures
References
-
- Rossi S, Miceli R, Messerini L, et al. Natural history of imatinib-naive GISTs: a retrospective analysis of 929 cases with long-term follow-up and development of a survival nomogram based on mitotic index and size as continuous variables. Am J Surg Pathol. 2011;35(11):1646–1656. - PubMed
-
- Hirota S, Isozaki K, Moriyama Y, et al. Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science. 1998;279(5350):577–580. - PubMed
-
- Heinrich MC, Corless CL, Duensing A, et al. PDGFRA activating mutations in gastrointestinal stromal tumors. Science. 2003;299(5607):708–710. - PubMed
-
- Oudijk L, Gaal J, Korpershoek E, et al. SDHA mutations in adult and pediatric wild-type gastrointestinal stromal tumors. Mod Pathol. 2013(3);26:456–463. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
