

Does Unprecedented ICU Capacity Strain, As Experienced During the COVID-19 Pandemic, Impact Patient Outcome?
- PMID: 35170537
- PMCID: PMC9112508
- DOI: 10.1097/CCM.0000000000005464
Does Unprecedented ICU Capacity Strain, As Experienced During the COVID-19 Pandemic, Impact Patient Outcome?
Abstract
Objectives: To determine whether patients admitted to an ICU during times of unprecedented ICU capacity strain, during the COVID-19 pandemic in the United Kingdom, experienced a higher risk of death.
Design: Multicenter, observational cohort study using routine clinical audit data.
Setting: Adult general ICUs participating the Intensive Care National Audit & Research Centre Case Mix Programme in England, Wales, and Northern Ireland.
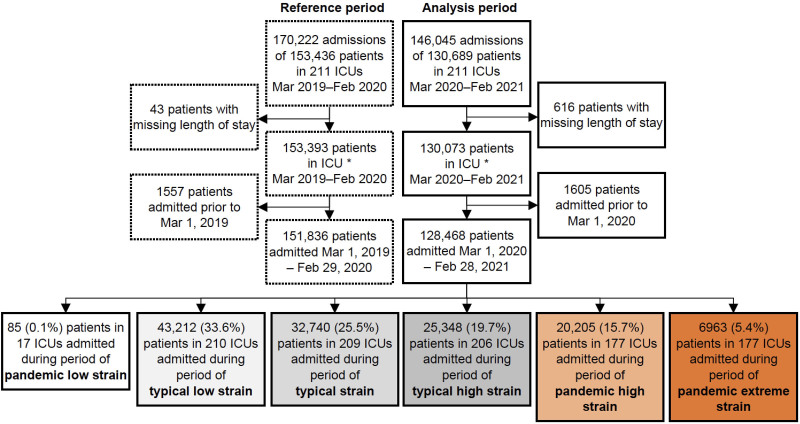
Patients: One-hundred thirty-thousand six-hundred eighty-nine patients admitted to 210 adult general ICUs in 207 hospitals.
Interventions: Multilevel, mixed effects, logistic regression models were used to examine the relationship between levels of ICU capacity strain on the day of admission (typical low, typical, typical high, pandemic high, and pandemic extreme) and risk-adjusted hospital mortality.
Measurements and main results: In adjusted analyses, compared with patients admitted during periods of typical ICU capacity strain, we found that COVID-19 patients admitted during periods of pandemic high or pandemic extreme ICU capacity strain during the first wave had no difference in hospital mortality, whereas those admitted during the pandemic high or pandemic extreme ICU capacity strain in the second wave had a 17% (odds ratio [OR], 1.17; 95% CI, 1.05-1.30) and 15% (OR, 1.15; 95% CI, 1.00-1.31) higher odds of hospital mortality, respectively. For non-COVID-19 patients, there was little difference in trend between waves, with those admitted during periods of pandemic high and pandemic extreme ICU capacity strain having 16% (OR, 1.16; 95% CI, 1.08-1.25) and 30% (OR, 1.30; 95% CI, 1.14-1.48) higher overall odds of acute hospital mortality, respectively.
Conclusions: For patients admitted to ICU during the pandemic, unprecedented levels of ICU capacity strain were significantly associated with higher acute hospital mortality, after accounting for differences in baseline characteristics. Further study into possible differences in the provision of care and outcome for COVID-19 and non-COVID-19 patients is needed.
Copyright © 2022 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Wilcox ME, Chong CA, Niven DJ, et al. : Do intensivist staffing patterns influence hospital mortality following ICU admission? A systematic review and meta-analyses. Crit Care Med 2013; 41:2253–2274 - PubMed
-
- Kahn JM, Goss CH, Heagerty PJ, et al. : Hospital volume and the outcomes of mechanical ventilation. N Engl J Med 2006; 355:41–50 - PubMed
-
- Gershengorn HB, Harrison DA, Garland A, et al. : Association of intensive care unit patient-to-intensivist ratios with hospital mortality. JAMA Intern Med 2017; 177:388–396 - PubMed
-
- Wilcox ME, Harrison DA, Patel A, et al. : Higher ICU capacity strain is associated with increased acute mortality in closed ICUs. Crit Care Med 2020; 48:709–716 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
