

Prognostic Value of Sequential Organ Failure Assessment (SOFA) Score in Critically-Ill Combat-Injured Patients
- PMID: 35171072
- PMCID: PMC9378752
- DOI: 10.1177/08850666221078196
Prognostic Value of Sequential Organ Failure Assessment (SOFA) Score in Critically-Ill Combat-Injured Patients
Abstract
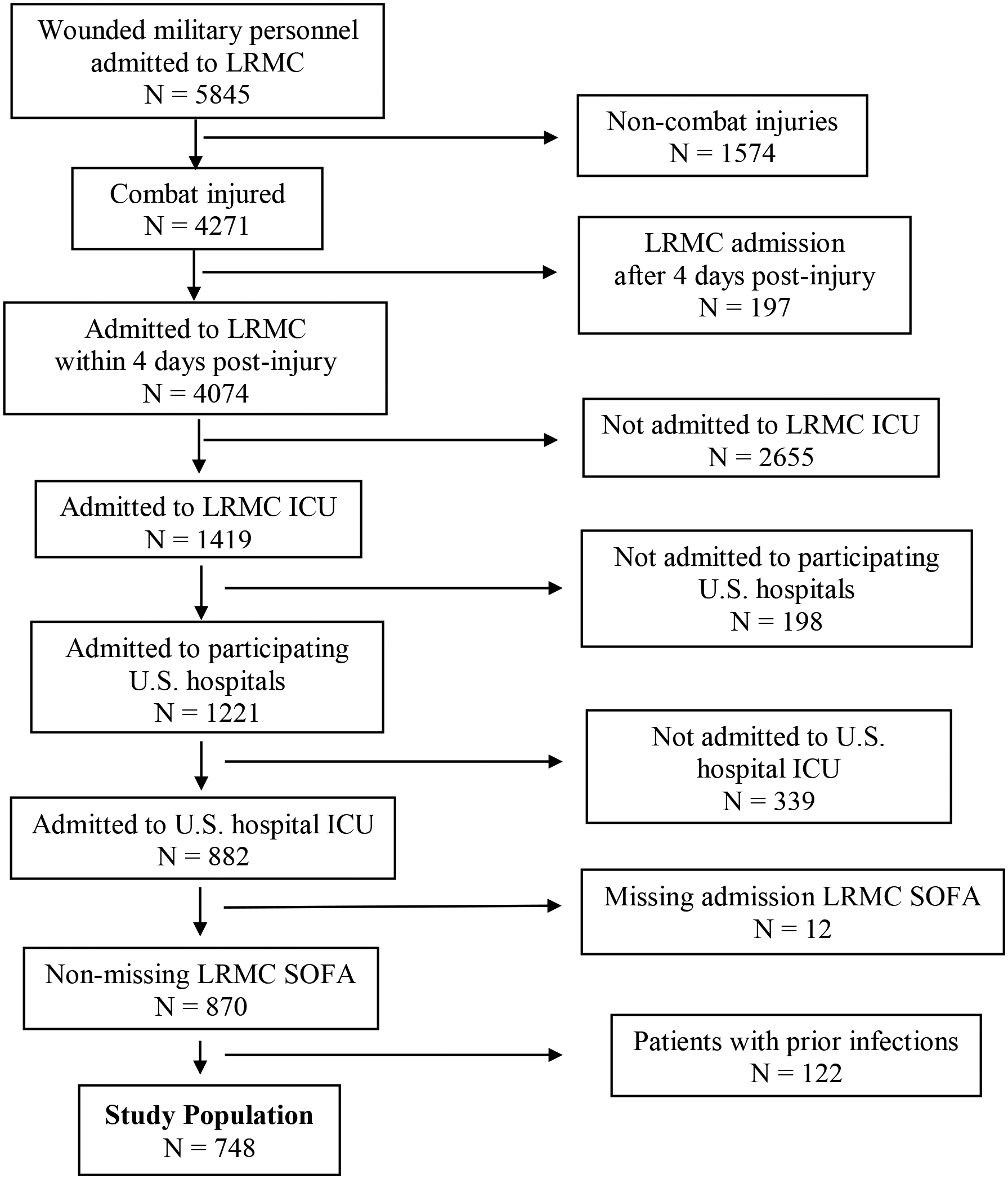
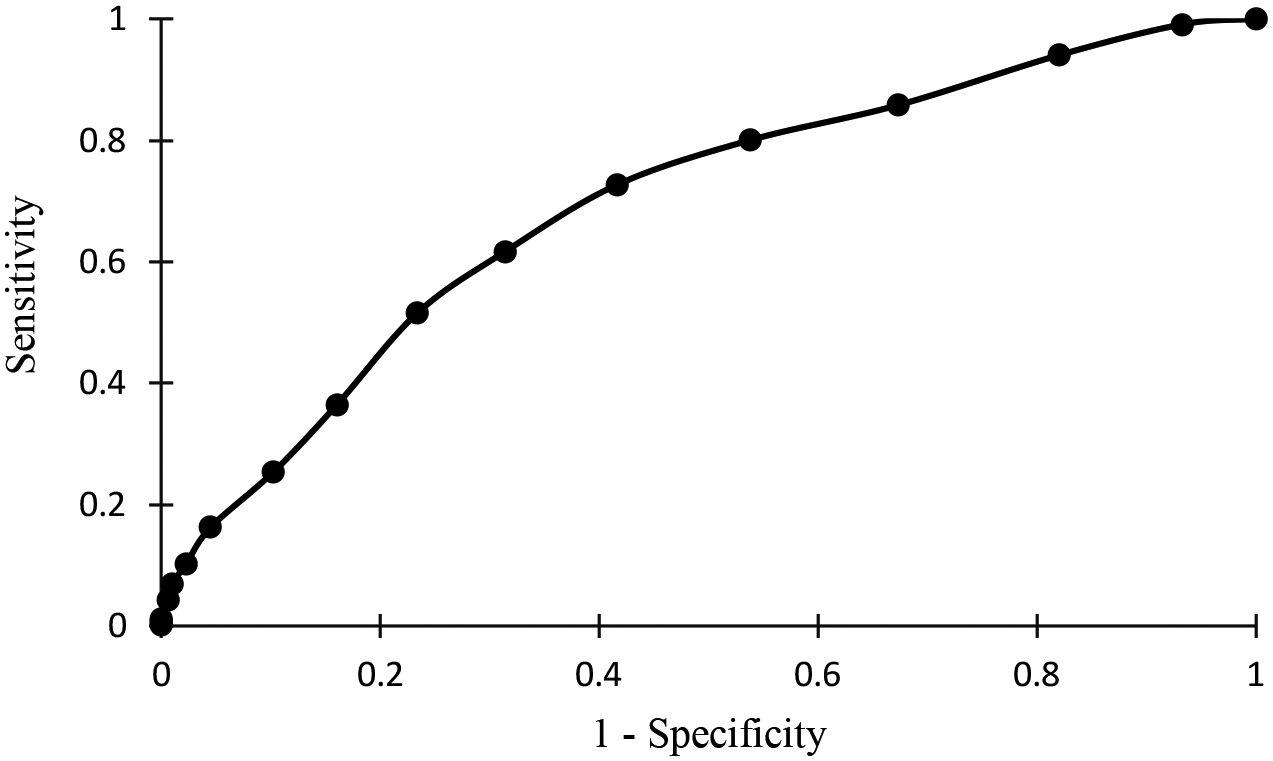
Background: Infection is a frequent and serious complication after combat-related trauma. The Sequential Organ Failure Assessment (SOFA) score has been shown to have predictive value for outcomes, including sepsis and mortality, among various populations. We evaluated the prognostic ability of SOFA score in a combat-related trauma population. Methods: Combat casualties (2009-2014) admitted to Landstuhl Regional Medical Center (LRMC; Germany) intensive care unit (ICU) within 4 days post-injury followed by transition to ICUs in military hospitals in the United States were included. Multivariate logistic regression was used to determine predictive effect of selected variables and receiver operating characteristic (ROC) curve analysis was used to evaluate overall accuracy of SOFA score for infection prediction. Results: Of the 748 patients who met inclusion criteria, 436 (58%) were diagnosed with an infection (32% bloodstream, 63% skin and soft tissue, and 40% pulmonary) and were predominantly young (median 24 years) males. Penetrating trauma accounted for 95% and 86% of injuries among those with and without infections, respectively (p < 0.001). Median LRMC admission SOFA score was 7 (interquartile range [IQR]: 4-9) in patients with infections versus 4 (IQR: 2-6) in patients without infections (p < 0.001). Thirty-day mortality was 2% in both groups. On multivariate regression, LRMC SOFA score was independently associated with infection development (odds ratio: 1.2; 95% confidence interval: 1.1-1.3). The ROC curve analysis revealed an area under the curve of 0.69 for infection prediction, and 0.80 for mortality prediction. Conclusions: The SOFA scores obtained up to 4 days post-injury predict late onset infection occurrence. This study revealed that for every 1 point increase in LRMC SOFA score, the odds of having an infection increases by a factor of 1.2, controlling for other predictors. The use of SOFA score in admission assessments may assist clinicians with identifying those at higher risk of infection following combat-related trauma.
Keywords: SOFA score; combat trauma; infection; infectious disease; severity score systems; trauma.
Conflict of interest statement
Figures
Similar articles
-
[Prognostic value of Charlson weighted index of comorbidities combined with sequential organ failure assessment score and procalcitonin in patients with sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Nov;31(11):1335-1339. doi: 10.3760/cma.j.issn.2095-4352.2019.11.005. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31898562 Chinese.
-
[The prognostic value of serum procalcitonin on severity of illness in non-sepsis critically ill patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016 Aug;28(8):688-93. doi: 10.3760/cma.j.issn.2095-4352.2016.08.004. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016. PMID: 27434557 Chinese.
-
[Comparison of four early warning scores in predicting the prognosis of critically ill patients in secondary hospitals].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Oct;35(10):1093-1098. doi: 10.3760/cma.j.cn121430-20230614-00441. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37873716 Chinese.
-
Pediatric Sequential Organ Assessment Score: A Comprehensive Review of the Prognostic Marker in the Pediatric Intensive Care Unit.Cureus. 2024 May 10;16(5):e60034. doi: 10.7759/cureus.60034. eCollection 2024 May. Cureus. 2024. PMID: 38854197 Free PMC article. Review.
-
Use of SOFA score in cardiac arrest research: A scoping review.Resusc Plus. 2020 Nov 3;4:100040. doi: 10.1016/j.resplu.2020.100040. eCollection 2020 Dec. Resusc Plus. 2020. PMID: 34223317 Free PMC article.
Cited by
-
Prehospital mSOFA Score for Quick Prediction of Life-Saving Interventions and Mortality in Trauma Patients: A Prospective, Multicenter, Ambulance-based, Cohort Study.West J Emerg Med. 2023 Sep;24(5):868-877. doi: 10.5811/westjem.59048. West J Emerg Med. 2023. PMID: 37788027 Free PMC article.
-
Risk factors for medical device-related pressure injury in ICU patients: A systematic review and meta-analysis.PLoS One. 2023 Jun 23;18(6):e0287326. doi: 10.1371/journal.pone.0287326. eCollection 2023. PLoS One. 2023. PMID: 37352180 Free PMC article.
-
Predictors and nomogram of in-hospital mortality in sepsis-induced myocardial injury: a retrospective cohort study.BMC Anesthesiol. 2023 Jul 7;23(1):230. doi: 10.1186/s12871-023-02189-8. BMC Anesthesiol. 2023. PMID: 37420185 Free PMC article.
References
-
- Murray CK, Hinkle MK, Yun HC. History of infections associated with combat-related injuries. J Trauma. 2008;64(3 Suppl):S221–S231. - PubMed
-
- Murray CK, Wilkins K, Molter NC, Li F, Yu L, Spott MA, Eastridge B, Blackbourne LH, Hospenthal DR. Infections complicating the care of combat casualties during operations Iraqi Freedom and Enduring Freedom. J Trauma. 2011;71(1 Suppl):S62–S73. - PubMed
-
- Yun HC, Blackbourne LH, Jones JA, Holcomb JB, Hospenthal DR, Wolf SE, Renz EM, Murray CK. Infectious complications of noncombat trauma patients provided care at a military trauma center. Mil Med. 2010;175(5):317–323. - PubMed
-
- Muckart DJ, Bhagwanjee S. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference definitions of the systemic inflammatory response syndrome and allied disorders in relation to critically injured patients. Crit Care Med. 1997;25(11):1789–1795. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
