

Associations Between Neuropsychiatric Symptoms and Neuropathological Diagnoses of Alzheimer Disease and Related Dementias
- PMID: 35171235
- PMCID: PMC8851371
- DOI: 10.1001/jamapsychiatry.2021.4363
Associations Between Neuropsychiatric Symptoms and Neuropathological Diagnoses of Alzheimer Disease and Related Dementias
Abstract
Importance: Understanding associations of Alzheimer disease (AD) and related dementias (ADRD) pathologies with common neuropsychiatric symptoms (NPS) may have implications for diagnosis and management.
Objective: To evaluate ADRD neuropathological diagnoses and NPS without consideration of clinical diagnosis.
Design, setting, and participants: This retrospective cohort study evaluated 1808 brains from 39 sites in the US National Alzheimer Coordinating Center v. 10 collection for participants among whom the Neuropsychiatric Inventory Questionnaire (NPIQ) was administered annually. Brain autopsy diagnoses of AD, Lewy body disease (LBD), cerebral amyloid angiopathy, frontotemporal lobar degeneration, cerebrovascular disease, hippocampal sclerosis, and no known pathology were examined. Autopsy data collected from January 2012 to January 2018 were deidentified and compiled into the publicly available v. 10 database. Data were analyzed from February 2021 to August 2021.
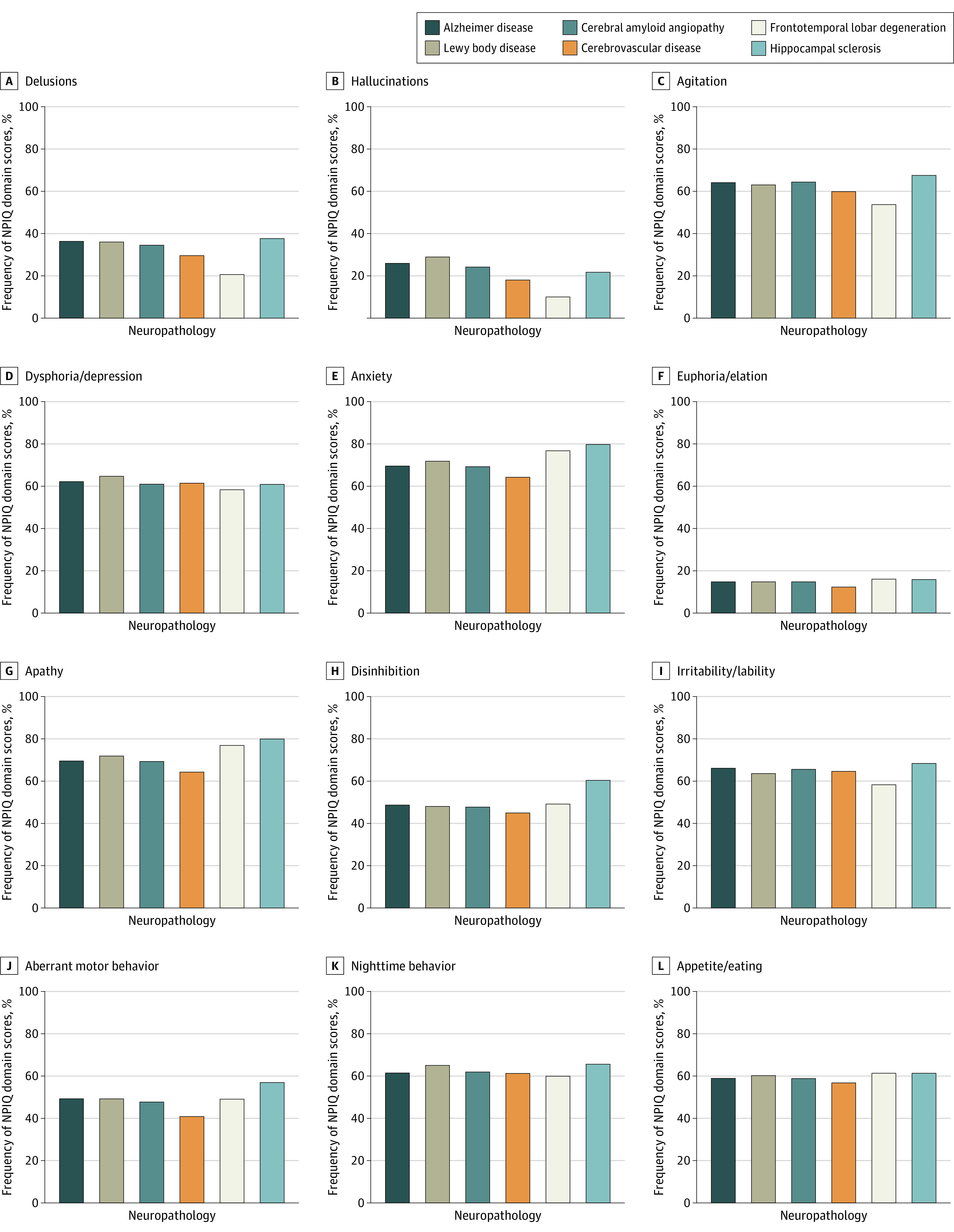
Main outcomes and measures: The primary outcome was NPIQ domain score, if present at any time point, and mean NPIQ domain score during follow-up was secondary. Associations of ADRD diagnoses with 12 NPIQ symptom domains were examined in regression analyses, correcting for multiple comparisons.
Results: The study sample of 1808 adults had a mean (SD) age of 80.0 (11.0) years, and 987 participants (54.6%) were male. Apathy was the most prevalent NPS, reaching 80% (203 of 254 individuals) in those with hippocampal sclerosis. Cerebrovascular disease showed few NPS associations. Frontotemporal lobar degeneration was associated with increased apathy, increased disinhibition, and decreased psychosis and agitation compared with AD. Hippocampal sclerosis was associated with increased apathy (odds ratio, 2.60; 95% CI; 1.86-3.66, false discovery rate controlled P < .001) and disinhibition (odds ratio, 2.15; 95% CI, 1.63-2.84; false discovery rate controlled P < .001). In multiple regression analyses that included concomitant neuropathologies, the main findings remained. More severe pathology was consistently associated with increased NPS (eg, LBD was associated with an increase in hallucinations from brain stem [β, 0.23; 95% CI, 0.07-0.76; P = .02] to limbic [β, 1.69; 95% CI, 1.27-2.27; P < .001] to neocortical [β, 4.49; 95% CI, 3.27-6.16; P < .001] pathology). Hallucinations were more common in participants with AD and LBD (168 of 534 [31.5%]) compared with those with AD without LBD (152 of 704 [21.6%]) and those with LBD without AD (23 of 119 [19.6%]).
Conclusions and relevance: In this cohort study of 1808 brains from the US National Alzheimer Coordinating Center, patients with LBD and AD showed a higher prevalence of hallucinations compared with those with LBD without AD. Neuropsychiatric symptom criteria of apathy and disinhibition in behavioral variant frontotemporal lobar degeneration were supported in this study. In hippocampal sclerosis, the findings of increased apathy and disinhibition merit further investigation. Severity of neuropathology was associated with NPS severity, indicating that NPS may reflect underlying ADRD pathology and highlighting the importance of diagnosing and treating NPS.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
