

Discrepant serological findings in SARS-CoV-2 PCR-negative hospitalized patients with fever and acute respiratory symptoms during the pandemic
- PMID: 35171507
- PMCID: PMC9088472
- DOI: 10.1002/jmv.27656
Discrepant serological findings in SARS-CoV-2 PCR-negative hospitalized patients with fever and acute respiratory symptoms during the pandemic
Abstract
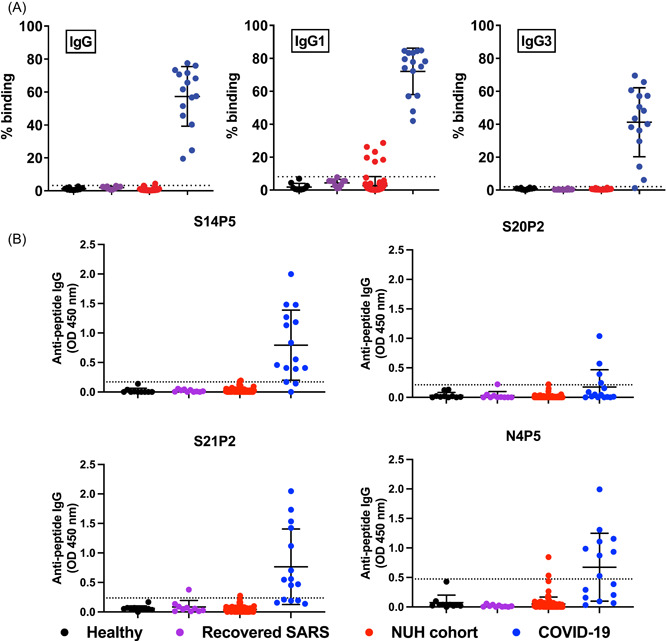
Coronavirus Disease 2019 (COVID-19) serology has an evolving role in the diagnosis of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. However, its use in hospitalized patients with acute respiratory symptoms remains unclear. Hospitalized patients with acute respiratory illness admitted to an isolation ward were recruited. All patients had negative nasopharyngeal swab polymerase chain reaction (PCR) for SARS-CoV-2. Serological studies using four separate assays (cPass: surrogate neutralizing enzyme-linked immunosorbent assay [ELISA]; Elecsys: N-antigen based chemiluminescent assay; SFB: S protein flow-based; epitope peptide-based ELISA) were performed on stored plasma collected from patients during the initial hospital stay, and a convalescent visit 4-12 weeks later. Of the 51 patients studied (aged 54, interquartile range 21-84; 62.7% male), no patients tested positive on the Elecsys or cPass assays. Out of 51 patients, 5 had antibodies detected on B-cell Epitope Assay and 3/51 had antibodies detected on SFB assay. These 8 patients with positive serological test to COVID-19 were more likely to have a high-risk occupation (p = 0.039), bacterial infection (p = 0.028), and neutrophilia (p = 0.013) during their initial hospital admission. Discrepant COVID-19 serological findings were observed among those with recent hospital admissions and bacterial infections. The positive serological findings within our cohort raise important questions about the interpretation of sero-epidemiology during the current pandemic.
Keywords: COVID-19; Singapore; serology.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
A patent application for the SFB assay has been filed (Singapore patent #10202009679 P: A Method Of Detecting Antibodies And Related Products). A patent application for SARS‐CoV‐2 linear B‐cell epitopes has been filed under the applications 10202002981 P and 10202004276 P. The remaining authors declare no conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
