

Mapping and ablation of left atrial roof-dependent tachycardias using an ultra-high resolution mapping system
- PMID: 35172730
- PMCID: PMC8851727
- DOI: 10.1186/s12872-022-02505-z
Mapping and ablation of left atrial roof-dependent tachycardias using an ultra-high resolution mapping system
Abstract
Background: Left atrial roof-dependent tachycardias (LARTs) are common macroreentrant atrial tachycardias (ATs). We sought to characterize clinical LARTs using an ultra-high resolution mapping system.
Methods: This study included 22 consecutive LARTs in 21 patients who underwent AT mapping/ablation using Rhythmia systems.
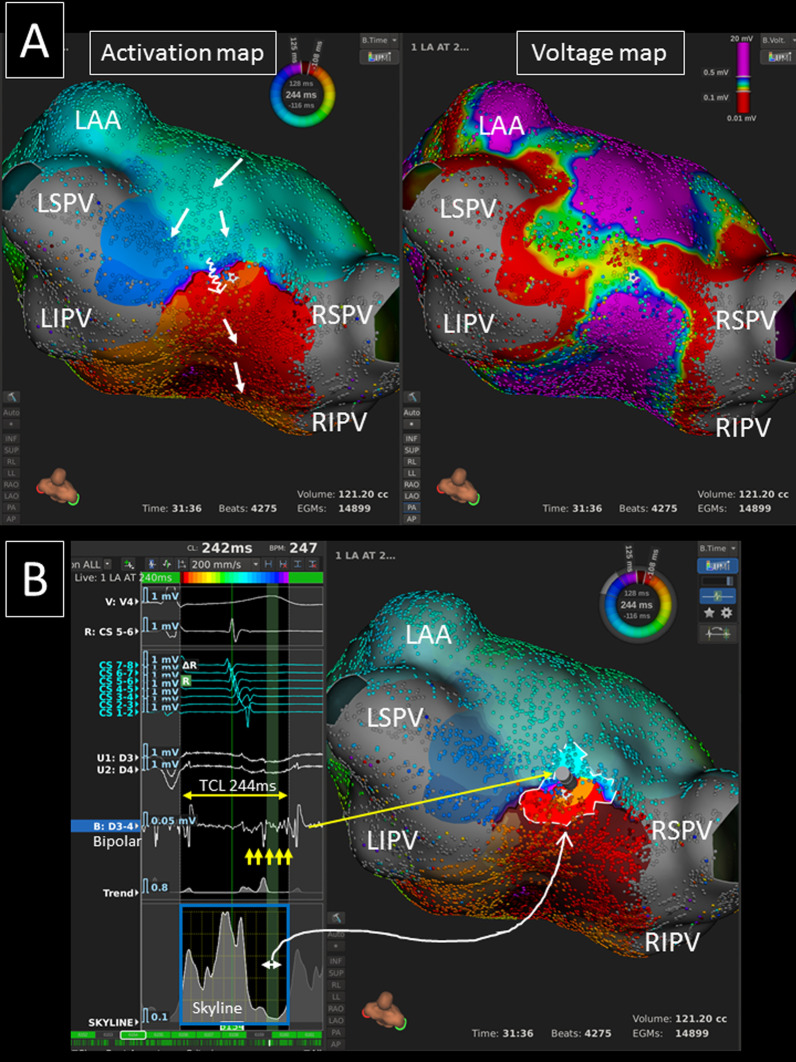
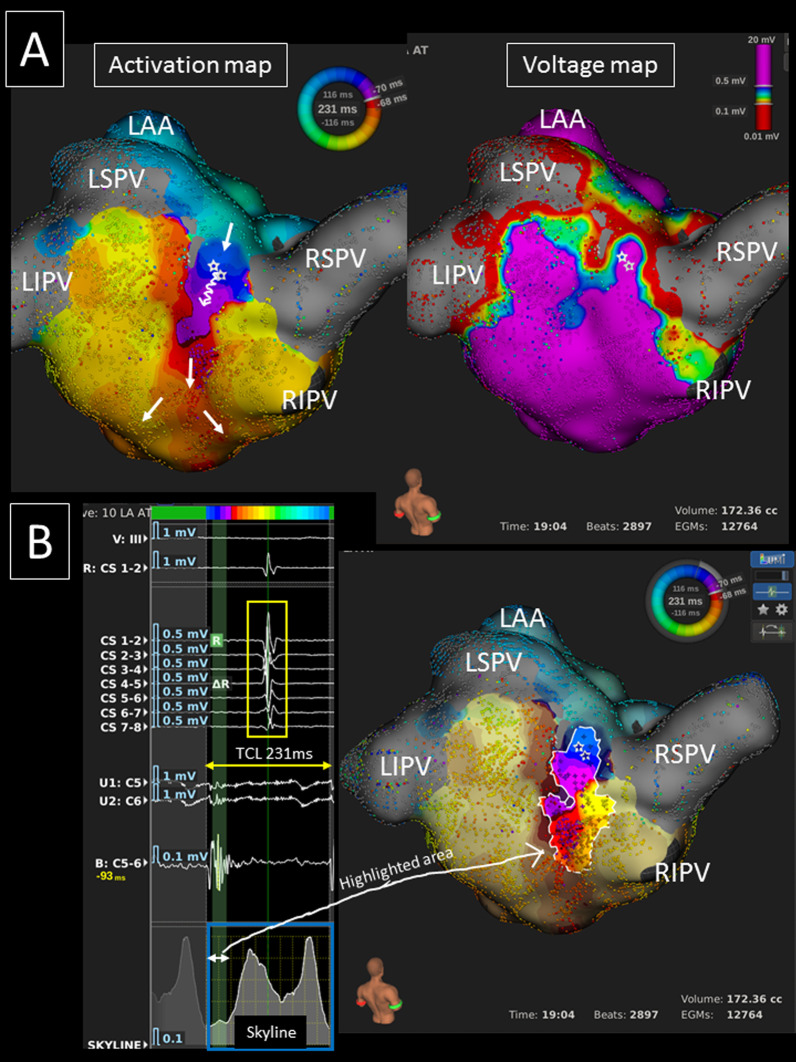
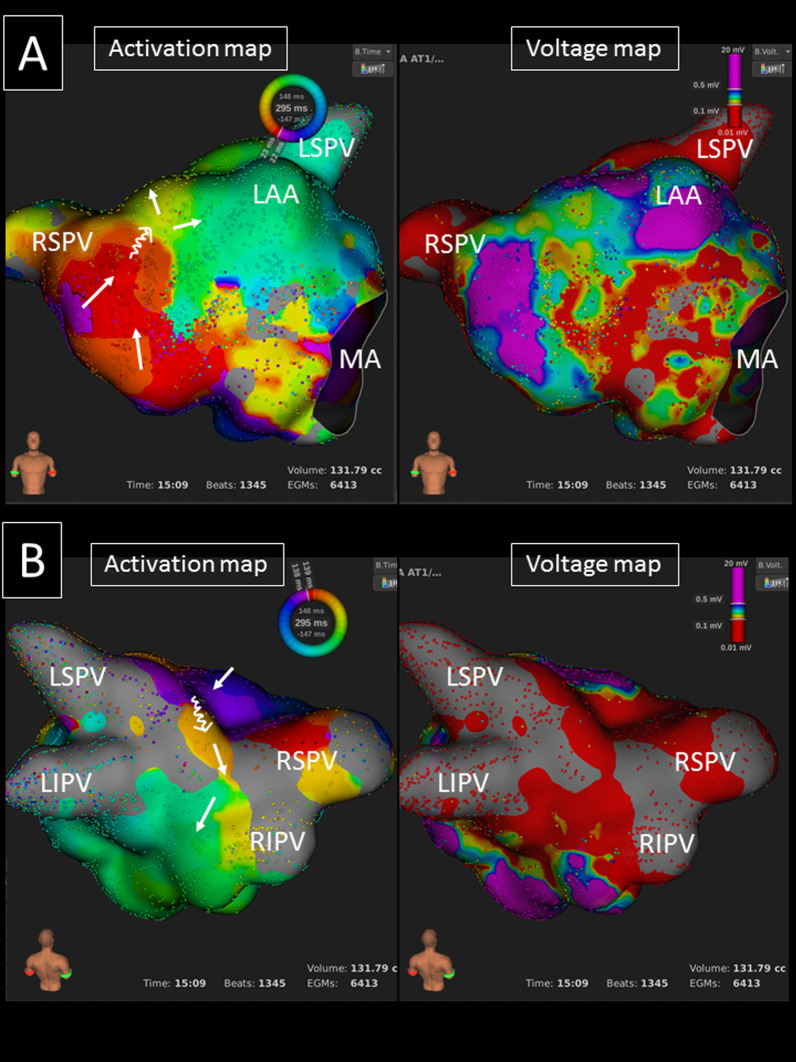
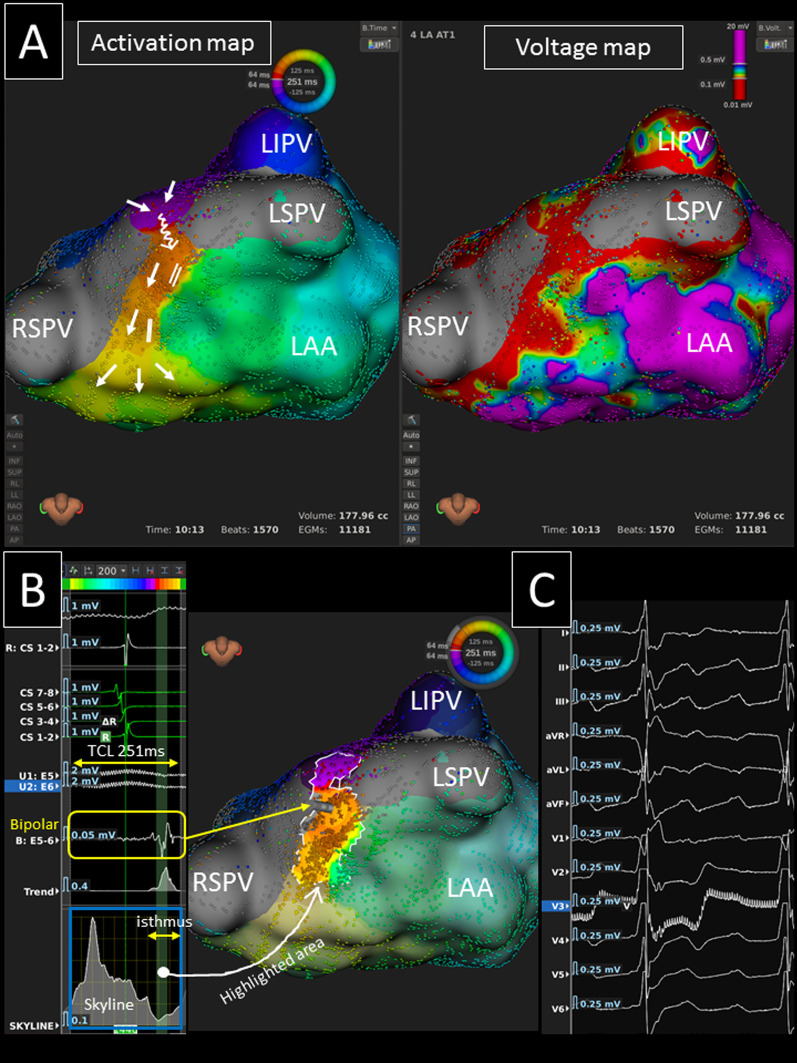
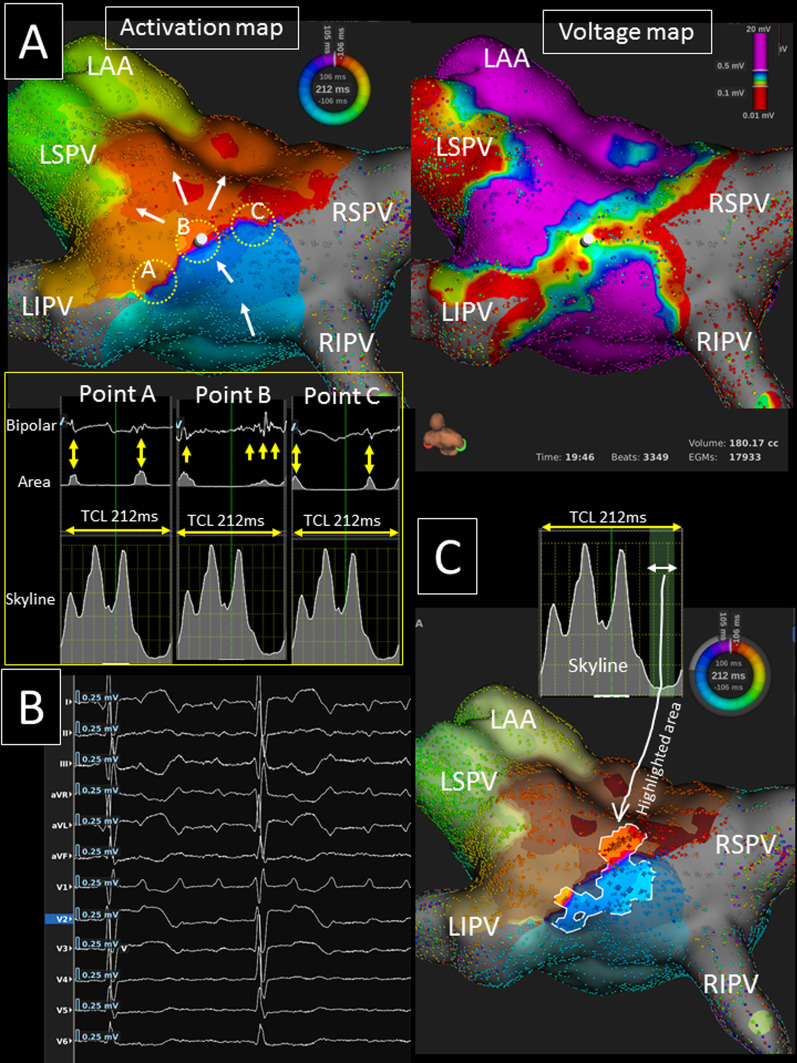
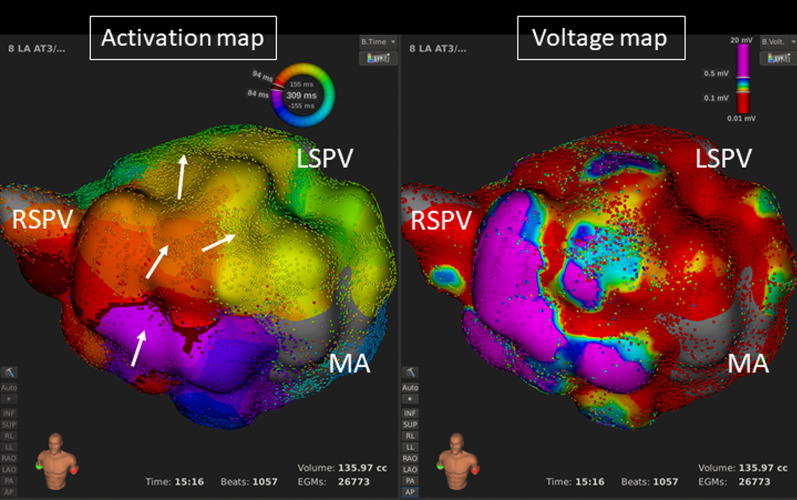
Results: Three, 13, 4, and 2 LART patients were cardiac intervention naïve (Group-A), post-roof line ablation (Group-B), post-atrial fibrillation ablation without linear ablation (Group-C), and post-cardiac surgery (Group-D), respectively. The mean AT cycle length was 244 ± 43 ms. Coronary sinus activation was proximal-to-distal or distal-to-proximal in 16 (72.7%) ATs. The activation map revealed 13 (59.1%) clockwise and 9 (40.9%) counter-clockwise LARTs. A 12-lead synchronous isoelectric interval was observed in 10/19 (52.6%) LARTs. The slow conduction area was identified on the LA roof, anterior/septal wall, and posterior wall in 18, 6, and 2 ATs, respectively. Twenty concomitant ATs among 13 procedures were also eliminated, and peri-mitral AT coexisted in 7 of 9 non-group-B patients. In group-B, the conduction gap was predominantly located on the mid-roof. Sustained LARTs were terminated by a single application and linear ablation in 6 (27.3%) and 9 (40.9%), while converting to other ATs in 7 (31.8%) LARTs. Complete linear block was created without any complications in all, however, ablation at the mid-posterior wall was required to achieve block in 4 (18.2%) procedures. During 14.0 (6.5-28.5) months of follow-up, 17 (81.0%) and 19 (90.5%) patients were free from any atrial tachyarrhythmias after single and last procedures.
Conclusions: The LART mechanisms were distinct in individual patients, and elimination of all concomitant ATs was required for the management.
Keywords: Atrial tachycardia; Catheter ablation; Roof line; Ultra-high resolution mapping.
© 2022. The Author(s).
Conflict of interest statement
Dr. Miyazaki belongs to the endowed departments of Medtronic, Boston, Abbott, and Japan Lifeline.
Figures
References
-
- Shah AJ, Jadidi A, Liu X, Miyazaki S, Forclaz A, Nault I, Rivard L, Linton N, Xhaet O, Derval N, Sacher F, Bordachar P, Ritter P, Hocini M, Jais P, Haissaguerre M. Atrial tachycardias arising from ablation of atrial fibrillation: a proarrhythmic bump or an antiarrhythmic turn? Cardiol Res Pract. 2010;2010:950763. doi: 10.4061/2010/950763. - DOI - PMC - PubMed
-
- Hocini M, Jaïs P, Sanders P, Takahashi Y, Rotter M, Rostock T, Hsu LF, Sacher F, Reuter S, Clémenty J, Haïssaguerre M. Techniques, evaluation, and consequences of linear block at the left atrial roof in paroxysmal atrial fibrillation: a prospective randomized study. Circulation. 2005;112:3688–3696. doi: 10.1161/CIRCULATIONAHA.105.541052. - DOI - PubMed
-
- Jaïs P, Matsuo S, Knecht S, Weerasooriya R, Hocini M, Sacher F, Wright M, Nault I, Lellouche N, Klein G, Clémenty J, Haïssaguerre M. A deductive mapping strategy for atrial tachycardia following atrial fibrillation ablation: importance of localized reentry. J Cardiovasc Electrophysiol. 2009;20:480–491. doi: 10.1111/j.1540-8167.2008.01373.x. - DOI - PubMed
-
- Mantziari L, Butcher C, Kontogeorgis A, Panikker S, Roy K, Markides V, Wong T. Utility of a novel rapid high-resolution mapping system in the catheter ablation of arrhythmias: an initial human experience of mapping the atria and the left ventricle. JACC Clin Electrophysiol. 2015;1:411–420. doi: 10.1016/j.jacep.2015.06.002. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
