

Global prevalence and burden of meal-related abdominal pain
- PMID: 35172840
- PMCID: PMC8851773
- DOI: 10.1186/s12916-022-02259-7
Global prevalence and burden of meal-related abdominal pain
Abstract
Background: Patients with disorders of gut-brain interaction (DGBI) report meal intake to be associated with symptoms. DGBI patients with meal-related symptoms may have more severe symptoms overall and worse health outcomes, but this subgroup has not been well characterized. We aimed to describe the global prevalence of meal-related abdominal pain and characterize this subgroup.
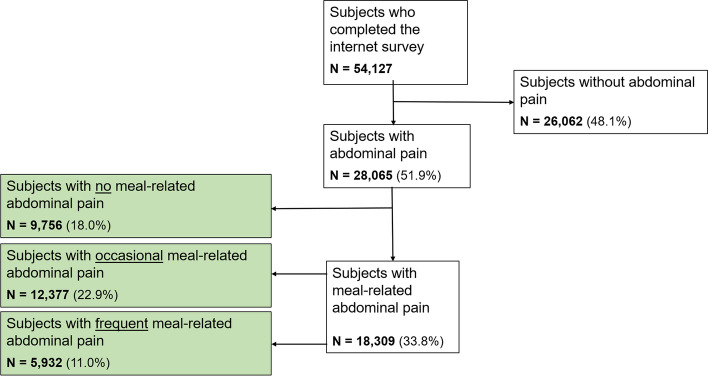
Methods: The data analyzed originated from the Internet survey component of the population-based Rome Foundation Global Epidemiology Study, completed in 26 countries (n = 54,127). Adult subjects were asked whether they had abdominal pain and how often this was meal-related. Respondents were categorized into "no," "occasional," and "frequent" meal-related abdominal pain groups based on 0%, 10-40%, and ≥50% of the pain episodes being meal-related, respectively. DGBI diagnoses, frequency of other GI symptoms, psychological distress, non-GI somatic symptoms, quality of life, and healthcare utilization were compared between groups. Mixed linear and ordinal regression was used to assess independent associations between psychological distress, non-GI somatic symptoms, quality of life, other GI symptoms, and meal-related abdominal pain.
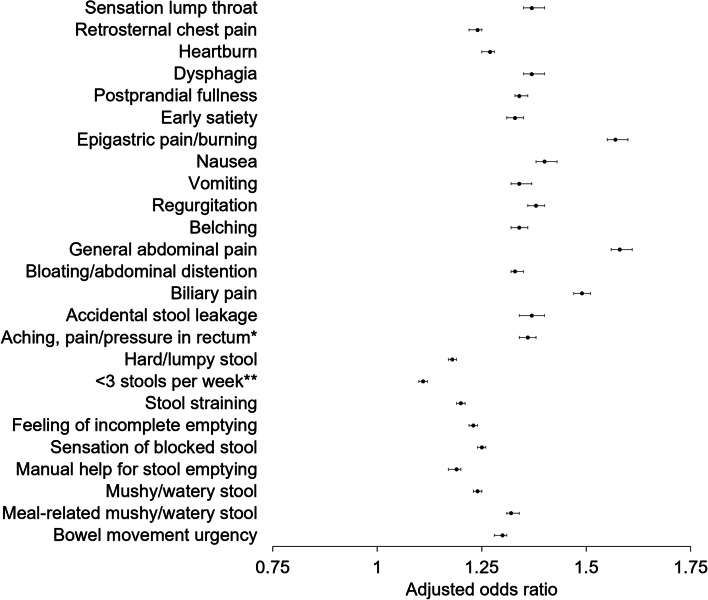
Results: Overall, 51.9% of the respondents reported abdominal pain in the last 3 months, and 11.0% belonged to the group with frequent meal-related abdominal pain, which included more females and younger subjects. DGBI diagnoses were more common in subjects with frequent meal-related abdominal pain, and the frequency of several GI symptoms was associated with having more frequent meal-related abdominal pain. Having meal-related abdominal pain more frequently was also associated with more severe psychological distress, non-GI somatic symptoms, and a poorer quality of life. The group with frequent meal-related abdominal pain also more often consulted a doctor for bowel problems compared to the other groups of meal-related abdominal pain.
Conclusion: Reporting frequent meal-related abdominal pain is common across the globe and associated with other GI and non-GI somatic symptoms, psychological distress, healthcare utilization, and a poorer quality of life. Individuals who frequently experience meal-related abdominal pain also more frequently fulfill the diagnostic criteria for DGBI. Assessing meal-related symptoms in all DGBI patients could be of major importance to improve and individualize symptom management.
Keywords: Burden; Disorders of the gut-brain interaction; Epidemiology; Food; Functional gastrointestinal disorders; Gastrointestinal symptoms; Global prevalence; Meal-related abdominal pain.
© 2022. The Author(s).
Conflict of interest statement
C.M. has served as a consultant/advisory board member for Kyowa Kirin, Norgine, Biocodex, MayolySpindler, Tillots, and Ipsen. S.S. has served as an advisory board member for Takeda and speaker for Viatris. H.T. has served as an advisory board member/consultant for Almirall and Shire. L.V.O. is assistant research professor of the KU Leuven Special Research Fund (Bijzonder Onderzoeksfonds, BOF). A.D.S. has served as a consultant for Lapidot Israel and AbbVie-Israel outside the submitted work. O.S.P. has received a research contract from the Rome Foundation during the conduct of the study and received a research contract from Glycom A/S and Royal DSM and personal fees from metaMe Health, outside the submitted work. J.T. has given scientific advice to Adare, AlfaWassermann, Allergan, Arena, Bayer, Christian Hansen, Clasado, Danone, Devintec, Falk, Grünenthal, Ironwood, Janssen, Kiowa Kirin, Menarini, Mylan, Neurogastrx, Neutec, Novartis, Noventure, Nutricia, Shionogi, Shire, Takeda, Theravance, Tramedico, Truvion, Tsumura, Zealand, and Zeria Pharmaceutical; received research support from Shire, Sofar, and Tsumura; and served on the Speakers Bureau for Abbott, Allergan, AstraZeneca, Janssen, Kyowa Kirin, Menarini, Mylan, Novartis, Shire, Takeda, Truvion, and Zeria Pharmaceutical, all outside the submitted work. M.S. has received grants and personal fees from Gkycom and Danone Nutricia Research; personal fees from Ironwood, Menarini, Biocodex, Adnovate, Arena, Tillotts, Kyowa Kirin, Takeda, Alimentary Health, AlfaSigma, and the Falk Foundation; and grants from Genetic Analysis AS, outside the submitted work. The remaining authors disclose no conflicts.
Figures



References
-
- Drossman DA. Functional gastrointestinal disorders: history, pathophysiology, clinical features and Rome IV. Gastroenterology. 2016. 10.1053/j.gastro.2016.02.032. - PubMed
-
- Sperber AD, Bangdiwala SI, Drossman DA, Ghoshal UC, Simren M, Tack J, et al. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome Foundation global study. Gastroenterology. 2021;160(1):99–114.e3. - PubMed
-
- Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol. 2012;10(7):712–21.e4. - PubMed
-
- Ford AC, Forman D, Bailey AG, Axon AT, Moayyedi P. Irritable bowel syndrome: a 10-yr natural history of symptoms and factors that influence consultation behavior. Am J Gastroenterol. 2008;103(5):1229–1239. - PubMed
-
- Hahn BA, Yan S, Strassels S. Impact of irritable bowel syndrome on quality of life and resource use in the United States and United Kingdom. Digestion. 1999;60(1):77–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
