

Subcutaneous cladribine to treat multiple sclerosis: experience in 208 patients
- PMID: 35173808
- PMCID: PMC8842147
- DOI: 10.1177/17562864211057661
Subcutaneous cladribine to treat multiple sclerosis: experience in 208 patients
Abstract
Objective: To report on safety and effectiveness of subcutaneous cladribine (Litak®) in multiple sclerosis (MS) patients.
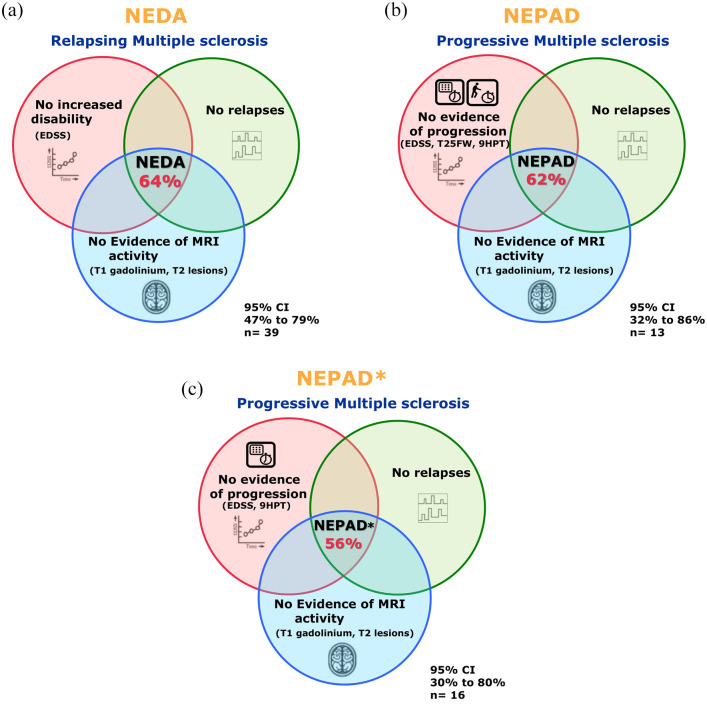
Methods: Litak® was offered to MS-patients irrespective of disease course. Litak® 10 mg was administered for 3-4 days during week 1. Based on lymphocyte count at week 4, patients received another 0-3 doses at week 5. A second course was administered 11 months later. Follow-up included adverse events, relapses, expanded disability status scale (EDSS), 9-hole-peg and Timed-25-foot-walking tests, no-evidence-of-disease-activity (NEDA), no-evidence-of-progression-or-active-disease (NEPAD), MRI, cerebrospinal fluid (CSF) neurofilament light chain (NfL), and lymphocyte counts.
Results: In all, 208 patients received at least one course of treatment. Age at baseline was 44 (17-72) years and EDSS 0-8.5. Cladribine was generally well tolerated. One myocardial infarction, one breast cancer, and three severe skin reactions occurred without long-term sequelae. Two patients died (one pneumonia, one encephalitis). Lymphopenia grade 3 occurred in 5% and grade 4 in 0.5%. In 94 out of 116 pwMS with baseline and follow-up (BaFU) data after two treatment courses, EDSS remained stable or improved. At 18 months, 64% of patients with relapsing MS and BaFU data (n = 39) had NEDA. At 19 months, 62% of patients with progressive MS and BaFU data (n = 13) had NEPAD. Of n = 13 patients whose CSF-NfL at baseline was elevated, 77% were normalised within 12 months.
Conclusions: Litak® was well tolerated. Effectiveness in relapsing MS appeared similar to cladribine tablets and was encouraging in progressive MS. Our data suggest cladribine may be safe and effective in MS-patients irrespective of their disease stage.
Keywords: NEDA; NEPAD; cladribine; disease-modifying treatment; multiple sclerosis; treatment access.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.A.P., S.D.T., Z.M., A.M., A.S., X.Z., O.Y., A.A., L.B., C.C., C.D., S.P., L.P.J., B.S. and S.W. have no conflicts of interest to declare. C.A.G. is a founder of NeuroCreare Ltd. J.M. has received honoraria and meeting support from Arvelle, Biogen, Novartis, Merck Serono, Roche and Sanofi Genzyme. C.B. has received travel costs and honoraria from Novartis, Genzyme, Teva and Biogen. K.C. has received honoraria and travel grants from Biogen, Sanofi-Genzyme and Roche. C.S.C. has received support for research, attendance of conferences, and consultancy from Biogen, GW Pharmaceuticals, Novartis, Teva, Merck, Morphosys, Roche, Sanofi Pasteur MSD and Sanofi Genzyme. R.A.F. has received honoraria and consultancy fees from Merck, TEVA, Novartis, Genzyme, GW Pharma, Allergan, Merz, Ipsen, and Biogen. R.A.F.’s current research activity is supported by the NIHR Biomedical Research Centre UCLH. L.F. has received consultancy fees from Biogen, Novartis, Roche and Genzyme. L.F. has received support for educational events from Biogen, Genzyme, Merck, Novartis, Teva, and the Neurology Academy. H.F. has received support from the Health Technology Assessment Programme (NIHR) and the UK MS Society. In the past 3 years, H.F. has been a local principal investigator for trials in MS funded by Novartis, Roche, and Biogen Idec and has taken part in advisory boards and consultancy for Biogen Idec, Merck, Novartis and Roche. B.G. has received personal compensation for consultancy from Merck, Roche, Biogen, Teva UK, and GW Pharma. B.G. has received unrestricted research grants from Biogen Idec, Merck, Bayer Healthcare, Teva UK, Novartis, and Genzyme. B.G. has received support for the attendance of clinical and research conferences from Biogen, Merck, Bayer Healthcare, Teva UK, Novartis, Genzyme, and CelGene. J.H. has received consultancy fees, meeting support, or grants to support clinical services or research from: Biogen Idec, Sanofi Genzyme, Janssen Cilag, Merck, Neurodiem, Novartis, Roche, Celegene, Oxford pharmagenesis. Z.K. has received honoraria and travel costs from Roche, Biogen and Novartis. M.M. has received travel support and speaker honoraria from Biogen Idec, Genzyme, Merck-Sereno, Novartis, Roche and Teva and consultation for Celgene, Merck-Serono, Novartis and Roche. O.P. has received speaking fees and travel expenses from, and/or served on advisory boards for, Biogen, Bayer, Celegene, Janssen, Merck Novartis, Roche, Sanofi and Teva. A.S. has received honoraria, travel grants and been a member of advisory boards for Biogen, Novartis, Teva, Celgene, Sanofi, and Merck. E.S. has received consulting fees and/ or support to attend academic meetings from Merck. E.T. has received honorarium for consulting work from Novartis, Merck, Biogen, and Roche. E.T. has received travel grants to attend or speak at educational meetings from Biogen, Merck, Roche, Takeda, and Novartis. B.P.T. has received honoraria, travel grants, and been a member of advisory boards for Biogen, Merck Serono, Novartis, Sanofi Genzyme, and Roche. M.M. has received honoraria and travel costs from Genzyme, AbbVie, Roche, and Novartis. S.G. has received honoraria from Biogen Idec, Sanofi Genzyme, Janssen Cilag, Merck, Neurodiem, Novartis, Roche, and Teva and grant support from ECTRIMS, Genzyme, Merck, National MS Society, Takeda, and UK MS Society. G.J. has received speaker honoraria from and is a member of advisory boards of AbbVie, Astellas, Celgene, and Novartis. G.G. has received honoraria and meeting support from AbbVie Biotherapeutics, Biogen, Canbex, Ironwood, Novartis, Merck, Merck Serono, Roche, Sanofi Genzyme, Synthon, Teva, and Vertex. He also serves as chief editor for Multiple Sclerosis and Related Disorders. D.B. has received compensation from InMuneBio, Lundbeck, Merck, Novartis, Rock, and Teva. K.S. has received research support from Biogen, Merck KGaA, and Novartis, speaking honoraria from, and/or served in an advisory role for, Amgen, Biogen, EMD Serono, Merck KGaA, Novartis, Roche, Sanofi-Genzyme, and Teva; and remuneration for teaching activities from AcadeMe, Medscape and the Neurology Academy.
Figures





References
-
- Gandey A. FDA rejects oral cladribine for multiple sclerosis. Medscape 2011, https://www.medscape.com/viewarticle/738239 (accessed 24 May 2021).
LinkOut - more resources
Full Text Sources
