

Efficacy of thoracoscopy combined with laparoscopy and esophagectomy and analysis of the risk factors for postoperative infection
- PMID: 35173853
- PMCID: PMC8829591
Efficacy of thoracoscopy combined with laparoscopy and esophagectomy and analysis of the risk factors for postoperative infection
Abstract
Objective: To explore the efficacy of thoracoscopy combined with laparoscopy (TCL) and esophagectomy in patients with esophageal carcinoma (EC) and analyze the risk factors for postoperative infection.
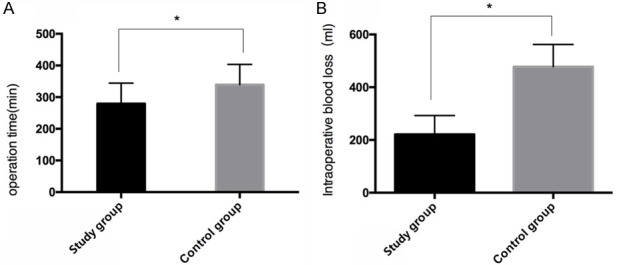
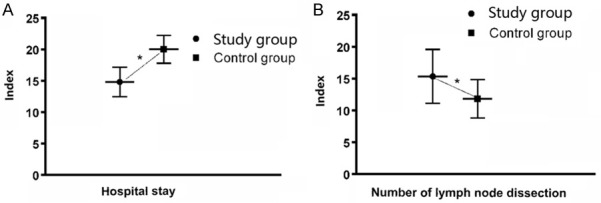
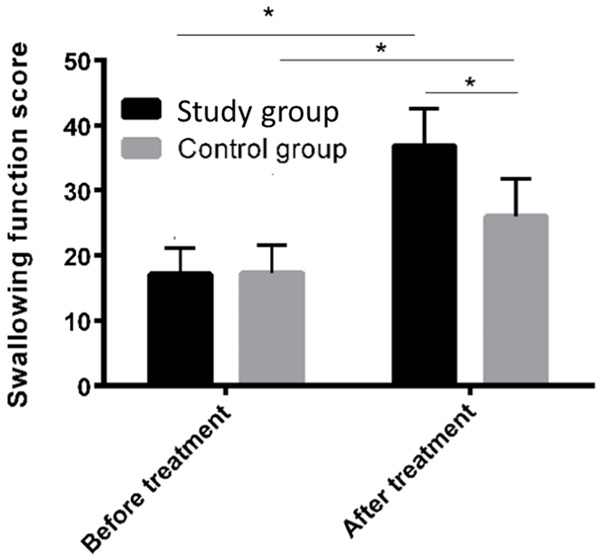
Methods: A total of 122 patients with EC admitted to our hospital were randomly divided into the study group (SG) and the control group (CG), with 61 patients in each group. Patients in the SG were treated with TCL, while patients in the CG were treated with traditional radical surgery for EC. The operation time, intraoperative blood loss, swallowing function, length of stay (LOS), number of lymph node dissections, postoperative infection rate, and quality of life in the first month after treatment were recorded and compared between the two groups. A logistic regression model was used to analyze the risk factors for postoperative infection.
Results: The operation time, intraoperative blood loss, LOS, and postoperative infection rate of the SG were significantly lower than those of the CG (all P<0.05). However, the number of lymph node dissections, swallowing function, and quality of life of patients in the SG were significantly higher than those in the CG, with statistically significant differences (all P<0.05). Postoperative hypoproteinemia, diabetes mellitus, and surgical mode were independent risk factors for postoperative infection in patients with EC (P<0.05).
Conclusion: Compared with traditional radical surgery for EC, TCL and resection can effectively reduce trauma, improve the lymph node dissection rate, promote postoperative recovery, and reduce postoperative infection, which is worthy of clinical application and promotion. Hypoproteinemia, diabetes mellitus, and surgical procedures are independent risk factors for postoperative infection in patients with EC. However, with improved medical technologies, the attention to and understanding of these high-risk factors can effectively improve postoperative infection in EC patients.
Keywords: Thoracoscopy combined with laparoscopy; postoperative infection; resection of esophageal carcinoma; risk factor.
AJTR Copyright © 2022.
Conflict of interest statement
None.
Figures
Similar articles
-
[Effects of robotic and laparoscopic-assisted surgery on lymph node dissection and short-term outcomes in patients with Siewert II adenocarcinoma of esophagogastric junction].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Feb 25;22(2):156-163. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 30799538 Clinical Trial. Chinese.
-
[Clinical application and analysis of single-port laparoscopic and thoracoscopic McKeown esophagectomy for esophageal cancer].Zhonghua Yi Xue Za Zhi. 2021 Aug 3;101(29):2316-2321. doi: 10.3760/cma.j.cn112137-20201215-03359. Zhonghua Yi Xue Za Zhi. 2021. PMID: 34333948 Chinese.
-
[Comparison of short-term and long-term efficacy between robot-assisted and thoracoscopy-laparoscopy-assisted radical esophageal cancer surgery].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Apr 25;23(4):390-395. doi: 10.3760/cma.j.cn.441530-20190327-00120. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32306608 Clinical Trial. Chinese.
-
Minimally invasive Ivor Lewis esophagectomy: Robot-assisted versus laparoscopic-thoracoscopic technique. Systematic review and meta-analysis.Surgery. 2021 Dec;170(6):1692-1701. doi: 10.1016/j.surg.2021.07.013. Epub 2021 Aug 11. Surgery. 2021. PMID: 34389164
-
Laparoscopic transhiatal esophagectomy for esophageal cancer.Am J Surg. 2005 Jul;190(1):69-74. doi: 10.1016/j.amjsurg.2004.12.004. Am J Surg. 2005. PMID: 15972176 Review.
Cited by
-
Assessing the predictive value of time-in-range level for the risk of postoperative infection in patients with type 2 diabetes: a cohort study.Front Endocrinol (Lausanne). 2025 Apr 15;16:1539039. doi: 10.3389/fendo.2025.1539039. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40303640 Free PMC article.
-
Analysis of risk factors affecting wound infection after open ankle fracture surgery.Medicine (Baltimore). 2025 Jul 11;104(28):e43191. doi: 10.1097/MD.0000000000043191. Medicine (Baltimore). 2025. PMID: 40660551 Free PMC article.
References
-
- Lin Y, Totsuka Y, Shan B, Wang C, Wei W, Qiao Y, Kikuchi S, Inoue M, Tanaka H, He Y. Esophageal cancer in high-risk areas of China: research progress and challenges. Ann Epidemiol. 2017;27:215–221. - PubMed
-
- Fuccio L, Mandolesi D, Farioli A, Hassan C, Frazzoni L, Guido A, de Bortoli N, Cilla S, Pierantoni C, Violante FS, Bazzoli F, Repici A, Morganti AG. Brachytherapy for the palliation of dysphagia owing to esophageal cancer: a systematic review and meta-analysis of prospective studies. Radiother Oncol. 2017;122:332–339. - PubMed
LinkOut - more resources
Full Text Sources