

Tuberculosis-Specific Antigen/Phytohemagglutinin Ratio Combined With GeneXpert MTB/RIF for Early Diagnosis of Spinal Tuberculosis: A Prospective Cohort Study
- PMID: 35174105
- PMCID: PMC8842995
- DOI: 10.3389/fcimb.2022.781315
Tuberculosis-Specific Antigen/Phytohemagglutinin Ratio Combined With GeneXpert MTB/RIF for Early Diagnosis of Spinal Tuberculosis: A Prospective Cohort Study
Abstract
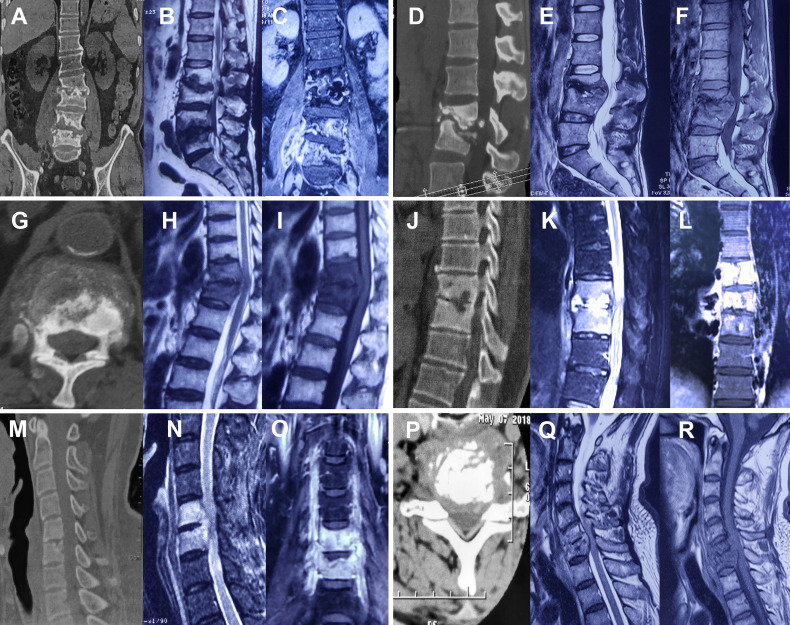
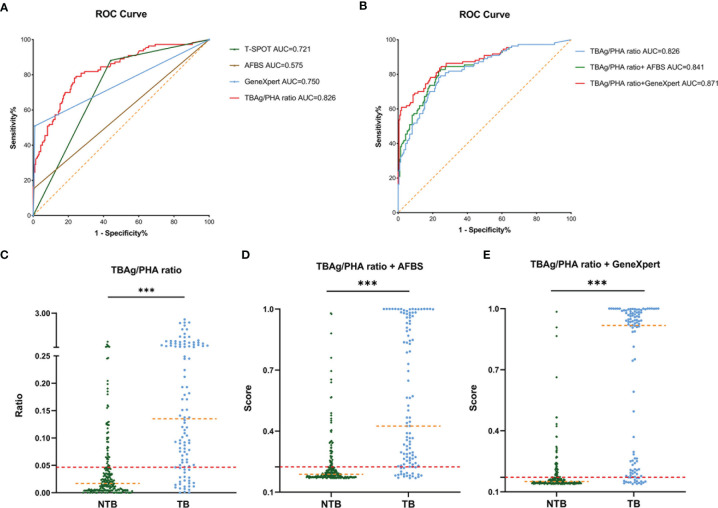
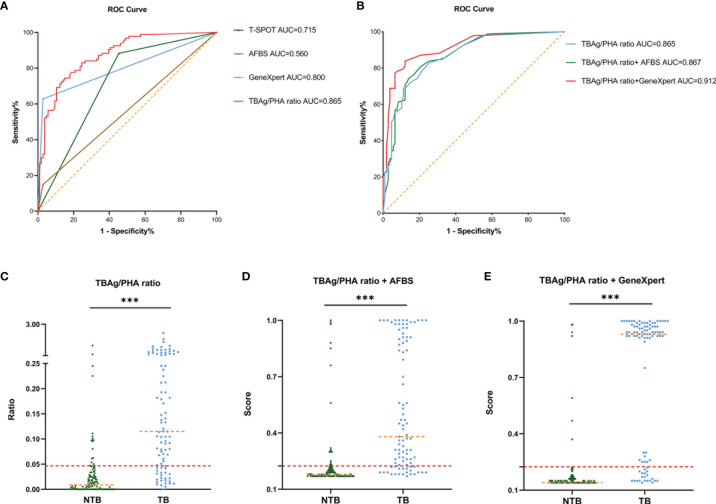
Spinal tuberculosis (TB), the most common form of musculoskeletal tuberculosis, is an infection-related disease globally, with paraplegia occurring in severe cases. Therefore, identification of spinal TB at an early stage is important for early intervention and eventual therapy. In this study, we conducted a prospective cohort study in routine clinical practice to investigate the diagnosis of different TB tests. A total of 519 patients were recruited based on the radiology of spinal TB. The diagnostic model was computed by regression analysis and was determined by receiver operating characteristic (ROC) curve analysis. Specificity, sensitivity, predictive value, likelihood ratio, and accuracy were also computed and compared. GeneXpert MTB/RIF showed a higher positive rate compared to that in the acid-fast bacilli smear and Mycobacterium culture. The results also showed that the Mycobacterium tuberculosis-specific antigen/phytohemagglutinin ratio in the T-SPOT assay had a good performance in the preoperative diagnosis and prediction of spinal TB. The diagnostic model based on the ratio of tuberculosis-specific antigen/phytohemagglutinin combined with GeneXpert MTB/RIF showed better efficiency for spinal TB diagnosis. In summary, the tuberculosis-specific antigen/phytohemagglutinin ratio combined with GeneXpert MTB/RIF could provide an early diagnosis of spinal TB.
Keywords: GeneXpert MTB/RIF; T-SPOT; spinal infection; spinal tuberculosis; tuberculosis diagnosis.
Copyright © 2022 Qi, Liu, Liu, Fang, Liu and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
COMPARISON OF GeneXpert MTB/RIF ASSAY WITH CONVENTIONAL AFB SMEAR FOR DIAGNOSIS OF PULMONARY TUBERCULOSIS IN NORTHEASTERN THAILAND.Southeast Asian J Trop Med Public Health. 2017 Mar;48(2):313-21. Southeast Asian J Trop Med Public Health. 2017. PMID: 29641882
-
Comparison of 3 diagnostic methods for pulmonary tuberculosis in suspected patients with negative sputum smear or no sputum.Medicine (Baltimore). 2024 Feb 9;103(6):e37039. doi: 10.1097/MD.0000000000037039. Medicine (Baltimore). 2024. PMID: 38335388 Free PMC article.
-
Diagnostic performance of GeneXpert MTB/RIF in detecting MTB in smear-negative presumptive TB patients.BMC Infect Dis. 2022 Apr 1;22(1):321. doi: 10.1186/s12879-022-07287-5. BMC Infect Dis. 2022. PMID: 35365080 Free PMC article.
-
Diagnostic accuracy of GeneXpert in the diagnosis of spinal tuberculosis: A systematic review and meta-analysis.Narra J. 2024 Aug;4(2):e925. doi: 10.52225/narra.v4i2.925. Epub 2024 Aug 13. Narra J. 2024. PMID: 39280292 Free PMC article.
-
Cost-Effectiveness of Currently Available Diagnostic Tools for Diagnosis of Pediatric Tuberculosis Under National Tuberculosis Elimination Program.Indian J Community Med. 2023 Jan-Feb;48(1):24-30. doi: 10.4103/ijcm.ijcm_471_22. Epub 2023 Feb 1. Indian J Community Med. 2023. PMID: 37082404 Free PMC article. Review.
Cited by
-
Analysis of the diagnostic efficacy of the QuantiFERON-TB Gold In-Tube assay for preoperative differential diagnosis of spinal tuberculosis.Front Cell Infect Microbiol. 2022 Sep 20;12:983579. doi: 10.3389/fcimb.2022.983579. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36204647 Free PMC article.
-
A predictive model for early clinical diagnosis of spinal tuberculosis based on conventional laboratory indices: A multicenter real-world study.Front Cell Infect Microbiol. 2023 Mar 24;13:1150632. doi: 10.3389/fcimb.2023.1150632. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37033479 Free PMC article.
-
Current landscape of exosomes in tuberculosis development, diagnosis, and treatment applications.Front Immunol. 2024 May 23;15:1401867. doi: 10.3389/fimmu.2024.1401867. eCollection 2024. Front Immunol. 2024. PMID: 38846947 Free PMC article. Review.
-
Unlocking the Diagnostic Potential: A Systematic Review of Biomarkers in Spinal Tuberculosis.J Clin Med. 2024 Aug 25;13(17):5028. doi: 10.3390/jcm13175028. J Clin Med. 2024. PMID: 39274240 Free PMC article. Review.
-
Clinical Value of Metagenomic Next-Generation Sequencing Using Spinal Tissue in the Rapid Diagnosis of Spinal Tuberculosis.Infect Drug Resist. 2023 May 29;16:3305-3313. doi: 10.2147/IDR.S410914. eCollection 2023. Infect Drug Resist. 2023. PMID: 37274359 Free PMC article.
References
-
- Alvarez-Uria G., Azcona J. M., Midde M., Naik P. K., Reddy S., Reddy R. (2012). Rapid Diagnosis of Pulmonary and Extrapulmonary Tuberculosis in HIV-Infected Patients. Comparison of LED Fluorescent Microscopy and the GeneXpert MTB/RIF Assay in a District Hospital in India. Tuberc. Res. Treat. 2012, 932862. doi: 10.1155/2012/932862 - DOI - PMC - PubMed
-
- Dorman S. E., Schumacher S. G., Alland D., Nabeta P., Armstrong D. T., King B., et al. . (2018). Xpert MTB/RIF Ultra for Detection of Mycobacterium Tuberculosis and Rifampicin Resistance: A Prospective Multicentre Diagnostic Accuracy Study. Lancet Infect. Dis. 18, 76–84. doi: 10.1016/S1473-3099(17)30691-6 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources